Anal Sacculectomy in Cats
Eliza Ruffner, DVM, Pine Valley Animal Hospital Wilmington, North Carolina
Melissa Daniels Fancher, DVM, Banfield Pet Hospital Clarksville, Tennessee
Courtney Sherman, DVM, Sherman Veterinary Services Cowan, Tennessee
Lauren Owens, DVM, SurgiCare Brandon, Florida
Karen M. Tobias, DVM, MS, DACVS, University of Tennessee
Perhaps because it is uncommon, misdiagnosed, or not reported, anal sac disease is not well documented in cats. Cats can have anal sac impaction, infection, abscessation, or neoplasia, any of which can result in discomfort or fecal obstruction. Closed anal sacculectomy is recommended to treat neoplasia or other conditions where wider margins may be necessary to remove all affected tissues or local contamination is a concern.
Clinical Signs
Clinical signs of feline anal sac disease include tenesmus, dyschezia, change in stool volume or consistency, perineal swelling or discomfort, scooting, recurrent constipation, abnormal tail carriage, ulceration, or draining tracts. Clinical signs can be confused with urinary tract problems or other constipation issues and may be missed by clients if signs are intermittent. In some cats with anal sac adenocarcinoma, the only sign is a palpable mass.1,2 Although anal sac disease can present at any age, neoplasia is most common in geriatric cats; in one report of 64 cats with anal sac adenocarcinoma, the median age was 12 years (range, 6–17 years).1
Diagnostic Findings
In cats with anal sac disease, diagnostics should start with a digital rectal examination. Because this procedure may be uncomfortable in patients with a small anus, appropriate restraint may require sedation or anesthesia. Full serum chemistry profile is recommended on presentation, as many cats with anal sac adenocarcinoma are geriatric and may have comorbidities. Unlike dogs, hypercalcemia is uncommon in cats with anal sac adenocarcinoma.1,2 If neoplasia is suspected, thoracic and abdominal radiography and abdominal ultrasonography should be requested to screen for metastatic disease in the lungs, liver, abdomen, and lymph nodes. Metastases have been suspected but have not been consistently confirmed in some cats with anal sac adenocarcinomas; true metastatic rate is unknown.1,2
Related Article: Anal Sacculectomy
If a mass is detected on digital rectal examination, samples obtained by fine-needle aspiration should be submitted for cytologic evaluation. Normal anal sac secretions in cats vary from light yellow–white or orange to tan or brown. The consistency may be thick and creamy or watery with inspissated material.3 Secretions in cats younger than 1 year of age are often watery. Microscopically, normal secretions contain large amounts of amorphous, basophilic material.3 Epithelial cells can be nucleated or nonnucleated with a mixed population of bacteria, predominantly gram-positive cocci. Healthy secretions may also have some neutrophils, monocytes, and yeast. Intracellular bacteria and erythrocytes are seldom identified in normal secretions.3
Cytology of inflamed anal sacs has not been described in cats; in a study comparing dogs with and without anal sac disease, there were no significant differences in numbers of bacteria or inflammatory cells.4 Cytologic appearance of anal sac adenocarcinoma can include clusters of papillary-shaped cells with poorly defined margins and malignant features (eg, nuclear or cellular pleomorphism, large nuclei, cytoplasmic vacuolization).5 Biopsy may be required for definitive diagnosis; excisional biopsy is recommended to lower risks for complications (eg, draining tract formation).
Anatomy
Blood supply is provided by branches of the caudal rectal artery and vein. Anal sacs are surrounded by the external anal sphincter muscle and perineal fat and are positioned lateral to the duct openings, which are located on pyramidal prominences of the skin at 120° and 240° (ie, 4 and 8 o’clock) lateral to the mucocutaneous junction. The locations of the caudal rectal nerves have not been well documented in cats.
Anal Sacculectomy
Surgical preparation includes clipping the perineal region and tail base. Analgesia can be provided preemptively with epidural administration of morphine (0.1 mg/kg) combined with saline to make 1-mL volume. The anal sacs should not be expressed if neoplasia is suspected. For patients with anal sacculitis, the sacs can be expressed and flushed, although this may be difficult because of small duct size. Because bacteria are present, prophylactic antibiotic therapy (eg, cefazolin) is recommended.
Anal sacculectomy is performed with the cat in perineal position and the tail pulled forward. The table edge should be padded to avoid femoral region compression. To reduce pressure on the diaphragm, the thorax can be elevated by placing a rolled towel behind the elbows; ventilation should be assisted intraoperatively.
Postoperative Care
After surgery, an Elizabethan collar should be applied for 1 to 2 weeks, and standard litter should be replaced with pelleted paper to prevent local contamination during healing. Analgesia can be provided via injectable or oral buprenorphine or an NSAID (eg, robenacoxib at 1 mg/kg PO q24h for up to 6 days). The safety margin of robenacoxib has only been evaluated in young, healthy cats6; therefore, as with other NSAIDs, caution is necessary with robenacoxib use in cats with compromised renal or hepatic function.
Complications include hemorrhage, swelling, infection, dehiscence, persistence of clinical signs, anal deformation or stricture, incontinence, or mass recurrence.1,2 Long-term complications include fecal incontinence, draining tract or fistula formation, or anal strictures.1,2,7 Although these complications are uncommon, rate of occurrence likely depends on surgeon skill and condition severity. In one study of cats with anal gland adenocarcinomas, median survival time was 3 months (range, 0–23 months). In those cats, death or euthanasia resulted from primary disease, presumptive metastasis, recurrence, or perceived poor outcome.1,2
Step-by-Step: Closed Anal Sacculectomy
What You Will Need
Standard surgical pack
3-0 nylon suture on a straight needle
Metzenbaum or blunt-tipped iris scissors
Babcock forceps
3-0 or 4-0 rapidly absorbable monofilament suture (eg, Monocryl, ethicon.novartis.us)
Foley catheter (optional)
Surgical tissue glue (optional)
Step 1
Place a purse-string suture at the mucocutaneous junction using 3-0 nylon on a straight needle; the suture line should be axial to the anal duct openings (arrow). Tighten to appose edges without necrosing tissues.
Author Insight
When placed appropriately, purse-string sutures allow duct openings to be catheterized during surgery to prevent duct occlusion or puncture, as needed.

Step 2
After the patient is positioned and aseptic preparation completed, make a 2-cm curvilinear incision over the anal sac, ~1–2 cm lateral to the opening. Identify the location of the anal sac by digital rectal palpation of the anal gland before placing a purse-string suture by inserting the tips of a closed hemostat through the duct into the sac during surgery.

Step 3
Bluntly dissect the subcutaneous fat away from the anal sphincter using Metzenbaum scissors. Spread blades parallel to the sphincter to reduce risk for tissue and vessel damage.

Step 4
Using Metzenbaum (A) or blunt-tipped iris scissors (B), dissect the external anal sphincter muscle away from the anal sac, keeping the blades parallel to the sac wall. Tenotomy scissors can have sharp tips that easily puncture the sac; however, they do not transect muscle as easily as Metzenbaum scissors do. The sac is easier to identify when it contains an instrument or other filling material (C).
Author Insight
If the duct is large enough, a small Foley catheter can be used to distend the sac. The catheter tip must be cut off or the balloon will not seat in the sac properly.



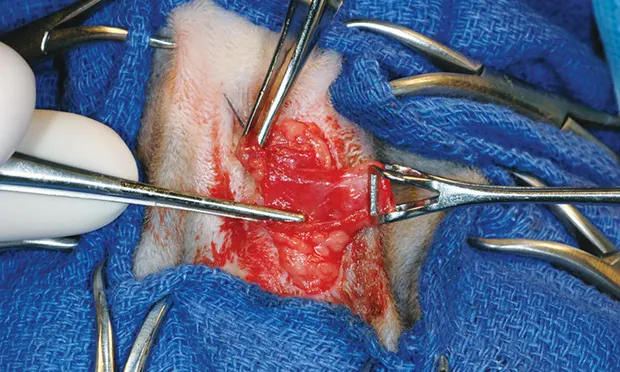
Step 5
Once the sac apex is exposed, grasp the sac’s end with Babcock forceps and retract laterally to expose the remaining muscle attachments.

Author Insight
When a hemostat is inserted, the pinkish-gray duct is more easily differentiated from attached muscle.

Step 6
Using the hemostat, identify the proximal end of the duct (A); ligate the duct with 3-0 rapidly absorbable monofilament suture, encircling the ligature as close to the duct opening as possible without compromising the external anal sphincter (B). Transect distal to the ligature, and submit the resected tissue for histologic evaluation.


Step 7
Appose subcutaneous tissues using simple interrupted sutures and skin with an intradermal pattern using 3-0 or 4-0 rapidly absorbable monofilament suture. If desired, place a thin layer of tissue glue over the incision line. Remove the purse-string suture. Swelling should be minimal the day after surgery.
