Removal of the Third Eyelid
Dennis E. Brooks, DVM, Ph.D., Diplomate ACVO
The third eyelid-nictitans or nictitating membrane-lies in the ventral-medial orbit of dogs, cats, and horses, where it physically protects the cornea and acts like a windshield wiper to distribute precorneal tear film.
It consists of a T-shaped piece of hyaline cartilage and a large seromucoid gland surrounding the base of the cartilage responsible for 25% to 40% of tear production. Conjunctiva lines the palpebral and bulbar sides of the third eyelid and contains lymphoid tissue on the bulbar side of the nictitans, suggesting some role in ocular immunoprotection. Goblet cells in the conjunctiva at the base of the nictitans produce the mucin layer of tear film. Movement of the nictitans is usually passive and determined by globe position in dogs and horses, although cats can also actively move the nictitans.
Overview
Frequent abnormalities of the third eyelid are protrusion, eversion of the nictitans cartilage, prolapse of the nictitans gland ("cherry eye"), foreign bodies behind the nictitans, enlargement of the gland of the third eyelid due to neoplasia or cyst formation, and hyperplasia of the bulbar lymphoid tissue (follicular conjunctivitis). The nonpigmented dorsal margin of the third eyelid may appear to be more pronounced than a third eyelid with a pigmented margin in large-breed dogs.


Squamous cell carcinoma of the third eyelid is present on the conjunctiva of a cat (left) and a horse (right).
The position of the third eyelid at the nasal canthus is determined by its spatial relationship to the globe and orbit. Prolapse or protrusion of the nictitans results from several causes. Passive protrusion of the nictitans occurs secondary to a lack of corneal support in enophthalmos and microphthalmos. Exophthalmos will result in increased forward pressure on the nictitans and its fascial attachments, causing nictitans protrusion.
Enophthalmos can be primary or secondary. The primary disorder is caused by active contraction of extraocular muscles if ocular pain is present. The secondary disorder results from decreased orbital contents, which may be due to dehydration, malnutrition, atrophy of orbital fat, or cachexia from debilitating systemic disease. Neurologic causes of enophthalmos are Horner's syndrome and dysautonomia.
Microphthalmos and phthisis bulbi result in small globes due to congenital and degenerative causes, respectively, and the nictitans protrudes due to a lack of physical support of the third eyelid with the globe. Adhesions of the bulbar or palpebral conjunctival surfaces (symblepharon) to the conjunctiva of the nictitans can cause chronic protrusion of the nictitans.
An increase in the volume of orbital contents from an orbital abscess or tumor causes exophthalmos, which in turn pushes the nictitans forward and causes third-eyelid protrusion. Neoplasia of the third eyelid or its gland can result in prominence or protrusion of the nictitans. Inflammatory diseases of the third eyelid, including nodular granulomatous episclerokeratitis and plasmoma, can also cause prominence of the third eyelid. Severe trauma to the nictitans may result in cartilage disfigurement and loss of third-eyelid tissue.
Tumors of the nictitans and its gland are common and often locally aggressive in dogs, cats, and horses. Tumors reported for the third eyelid and nictitans gland include adenoma, adenocarcinoma, squamous cell carcinoma, mastocytoma, papilloma, hemangioma, melanoma, and lymphoma. Squamous cell carcinoma and melanoma of the third eyelid can be aggressive and have metastatic potential in animals.
Surgical removal of the third eyelid is strictly reserved for neoplasia of the nictitans and its gland or for traumatic injury severe enough to interfere with function of the nictitans and globe; removal for "cherry eyes" or cosmetic reasons is inappropriate. The free margin of the third eyelid alone may be removed, and the rest of the nictitans and its gland preserved, in surgical therapy of small nictitans tumors that involve only the margin.
A basic surgical technique for removal of the entire nictitans and its gland is described here. General anesthesia is required to perform this relatively short procedure in dogs and cats, while heavy sedation and sensory nerve blocks are adequate in standing horses. Complications, although rare, include orbital fat prolapse, hemorrhage, KCS or superficial keratitis, entropion, conjunctivitis, and infection. KCS in American cocker spaniels and English bulldogs can be related to nictitans removal in some cases.
Step-by-Step: How to Remove the Third Eyelid
Step 1
An adenoma of the third-eyelid gland protrudes above the dorsal margin of the third eyelid. The surgical site is prepared and draped. A wire lid speculum aids exposure of the nictitans during the procedure.

Step 2
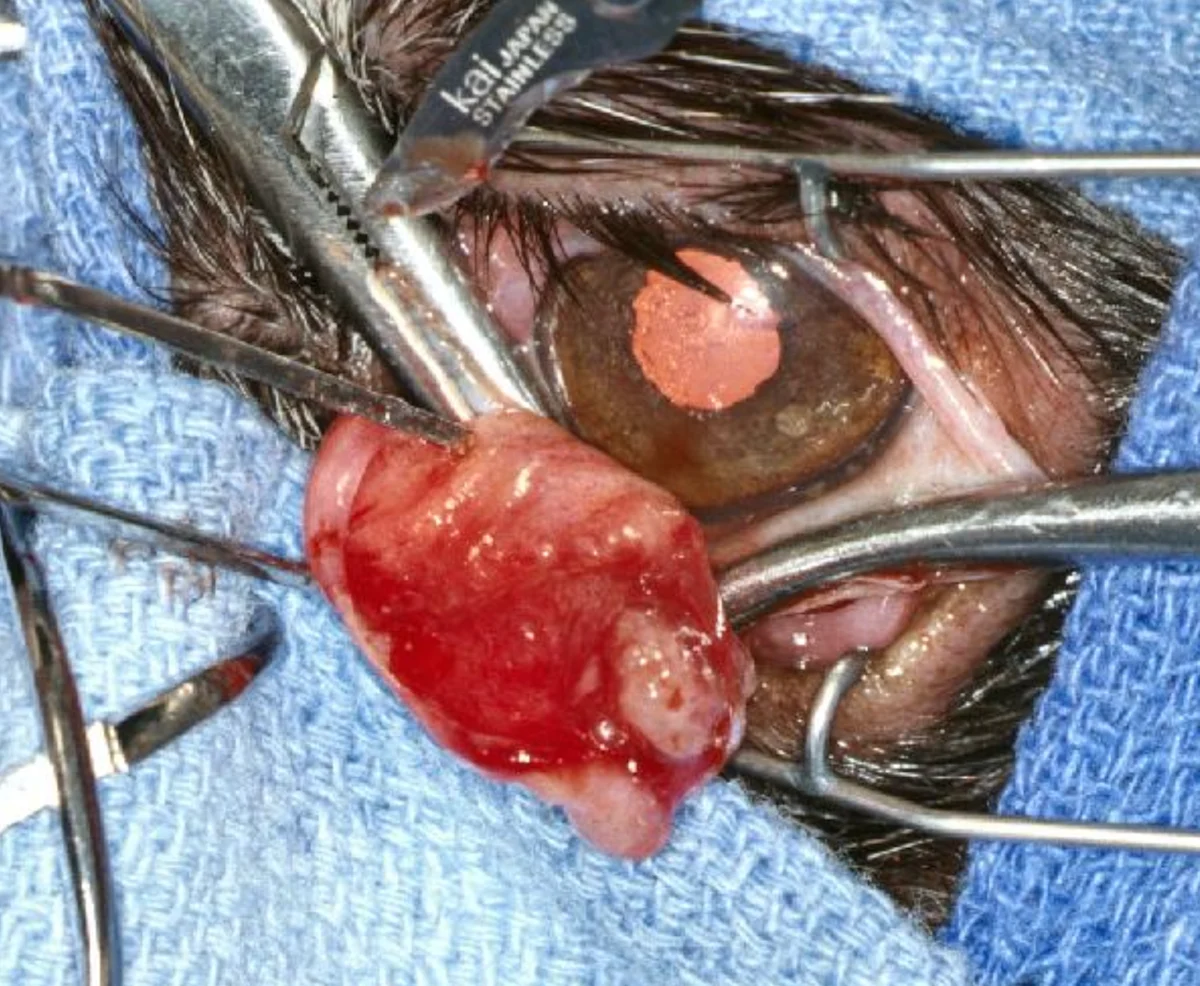
Gently grasp the dorsal margin of the third eyelid with small hemostats or Bishop Harmon-toothed forceps. Pull the third eyelid up and outward; this makes the tumor more easily observed. Position and clamp a curved hemostat below the mass halfway across the base of the third eyelid at the most ventral region of the third eyelid; this minimizes postoperative hemorrhage.

Step 3
Position and clamp a second curved hemostat opposite the first hemostat, such that the base of the third eyelid is completely clamped.

Step 4
Use a no. 15 blade to incise the third eyelid along the hemostats.
Procedure Pearl
Surgical removal of the third eyelid is strictly reserved for neoplasia of the nictitans and its gland or for traumatic injury severe enough to interfere with function of the nictitans and globe; removal for "cherry eyes" or cosmetic reasons is inappropriate.

Step 5
Continue the incision along the hemostats to remove the glandular tumor and third eyelid.

Step 6
Continue the incision from the other side.
Step 7
Leave the hemostats clamped for 2 to 3 minutes after nictitans removal.

Step 8
The conjunctival area at the base of the third eyelid can be carefully sutured with 5-0 Vicryl, or not sutured and left to granulate. Postoperative hemorrhage is minor in my experience but can be controlled with pressure and light cautery. Topical antibiotics are indicated for 5 to 7 days after surgery.
