Epidemiology of Pyloric Outflow Obstructions
Pyloric outflow tract obstruction secondary to an anatomic abnormality can be congenital or acquired. Hypertrophy of the muscularis layer is most common in congenital cases, although the mucosal layer can also be involved.1,2 Brachycephalic dogs are overrepresented for congenital obstructions, and acquired obstructions are reported more often in middle-aged to older small-breed dogs.3,4 Most dogs with this condition have a history of chronic vomiting.2-4 Differential diagnoses include gastroesophageal reflux/motility disorders, outflow tract foreign body obstructions, and gastric neoplasia.
Surgical Treatment for Pyloric Outflow Obstructions
Various surgical interventions have been described, including Fredet-Ramstedt pyloromyotomy (Figure 1), Heineke-Mikulicz pyloroplasty (no image), and Y-U pyloroplasty (Figure 2).5,6

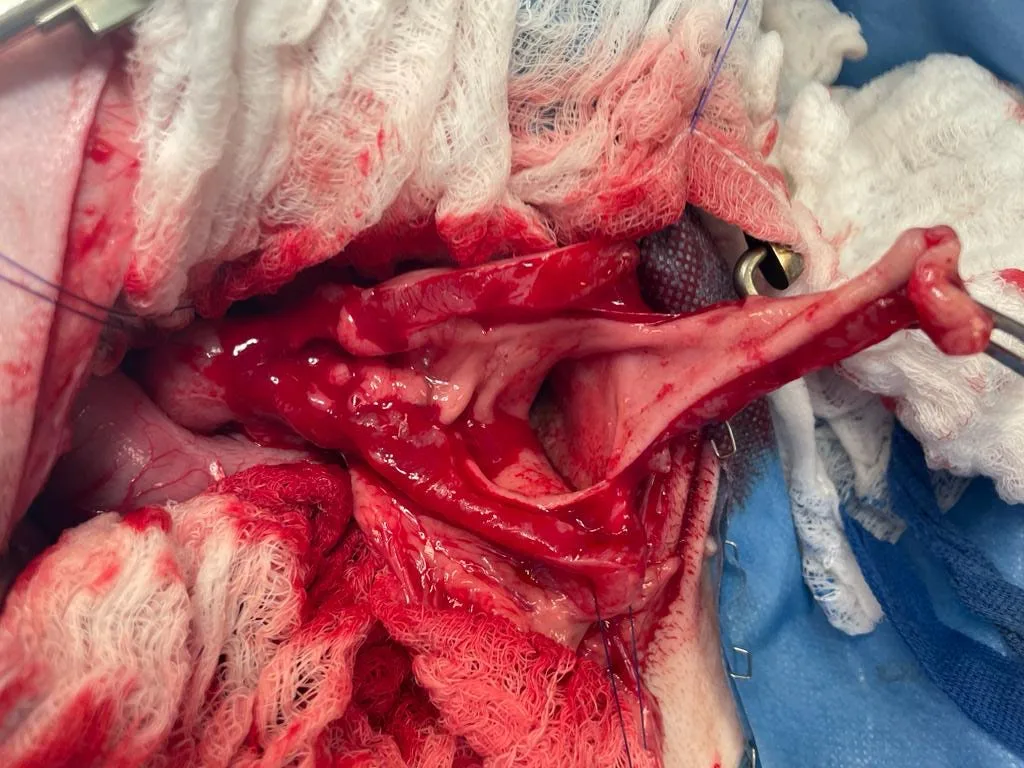
FIGURE 1 The pylorus is incised with a partial-thickness incision (as is performed with Fredet-Ramstedt pyloromyotomy) through the serosa and muscularis, showing the severely thickened muscularis layer with the underlying mucosa–submucosa exposed. Note: The duodenum is to the left and the body of the stomach is to the right of the image.

FIGURE 2 View of the stomach (top of the image) and duodenum (bottom of the image) prior to incision, with a Y overlay showing where the Y-U pyloroplasty will be performed. The stem of the Y is on the antimesenteric border of the proximal descending duodenum, the pylorus is at the intersection of all 3 arms, and the pyloric antrum of the stomach is outlined by the 2 arms of the Y.
Fredet-Ramstedt pyloromyotomy involves a longitudinal partial-thickness incision of the thickened muscular layer that allows protrusion of the mucosa–submucosa layer through the incision. Heineke-Mikulicz pyloroplasty (ie, transverse pyloroplasty) involves making a longitudinal full-thickness incision through the pylorus and closing transversely. Y-U pyloroplasty involves making a Y-shaped full-thickness incision (with the stem extending along the antimesenteric border of the proximal descending duodenum and the arms curving along the ventral margins of the pyloric antrum), advancing the normal gastric pyloric antrum wall across the incised thickened pylorus, and closing the incision in a U-shape (Figures 3-6). Heineke-Mikulicz pyloroplasty and Y-U pyloroplasty permit full-thickness gastric biopsy and thus definitive confirmation of benign pyloric hypertrophy. Surgical widening of the outflow tract usually results in rapid improvement of clinical signs and good prognosis.

FIGURE 3 Y-shaped incision made for Y-U pyloroplasty, with the stem starting several centimeters into the proximal descending duodenum, full-thickness extension through the pylorus, and the arms curving to either side of the pyloric antrum. On completion of the armed incisions, the pyloric antrum is elevated. Note: The duodenum is to the left and the body of the stomach is to the right of the image.