Chronic Pancreatitis in Dogs
Harry Cridge, MVB, MS, PG Cert Vet Ed, DACVIM (SAIM), DECVIM-CA, FHEA, MRCVS, Michigan State University
Chronic pancreatitis is an inflammatory condition that can lead to irreversible damage to both the exocrine and endocrine pancreas. Unlike acute pancreatitis, which manifests as a sudden severe illness, chronic pancreatitis often progresses insidiously or with mild waxing and waning clinical signs that can make diagnosis and management challenging.
Prevalence, Signalment, & Causes
Incidence/Prevalence
One study revealed microscopic evidence of pancreatitis in 34% of randomly selected necropsy cases originating from primary care clinics in the United Kingdom, and a second study reported evidence of pancreatitis in up to 64% of cases.1,2
These studies likely overestimate prevalence in dogs but highlight the potential frequency of chronic pancreatic inflammation, despite the overall uncommon nature of its recognition in clinical practice, suggesting underdiagnosis.
Acute-on-chronic presentations are also likely underdiagnosed as a result of an overlooked underlying chronic component.
In a study, ≈40% of dogs diagnosed with fatal acute pancreatitis had features of chronicity on histopathology.3
Signalment
Breed Predisposition
In the United States, nonsporting and toy breeds appear to be at greatest risk, with Labrador retrievers, boxers, miniature schnauzers, collies, and dachshunds seemingly overrepresented.4
In the United Kingdom, boxers, collies, and spaniels appear overrepresented.1,5-7
A unique clinicopathologic disease pattern similar to immunoglobulin G4 (IgG4)–related disease has been identified in English cocker spaniels.1,5-7
Any breed can be affected.
Age
Middle-aged to older dogs appear to be predisposed.
Causes & Risk Factors
The cause of chronic pancreatitis is thought to be idiopathic in most cases; however, risk factors for acute pancreatitis could be potential risk factors for chronic or recurrent pancreatitis.
Potential causes for acute pancreatitis include8:
Dietary factors (eg, high-fat diet, ingestion of unusual food items or table scraps)
Drug exposure (eg, L-asparaginase, phenobarbital, potassium bromide)
Underlying endocrinopathies (eg, diabetes mellitus, hyperadrenocorticism, hypothyroidism)
Hypertriglyceridemia
Miscellaneous factors (eg, obesity)
Clinical Presentation
Patients with chronic pancreatitis often have mild GI upset, hyporexia, lethargy, and abdominal discomfort.4,5
Postprandial pain may also be noted, particularly in hindsight, when appropriate analgesia restores normal comfort levels.
Concurrent disease, particularly secondary consequences of exocrine pancreatic insufficiency (EPI; eg, diabetes mellitus [DM]), may alter clinical presentation.
Dogs with EPI may have poor coat quality, weight loss despite a good appetite, and loose stools.9
Dogs with DM may have polyuria and polydipsia in addition to weight loss.
Differential Diagnoses
Differential diagnoses for chronic pancreatitis include, but are not limited to, chronic enteropathies, hypoadrenocorticism, and low-grade hepatic and renal disease.
English cocker spaniels with IgG4-related disease may have clinical signs of concurrent keratoconjunctivitis sicca, protein-losing nephropathy, and anal sac disease.10
Diagnosis
Definitive Diagnosis
Diagnosis of chronic pancreatitis is challenging and largely based on overall assessment of patient history, clinical signs, ultrasound findings, results of pancreas-specific lipase testing, and ruling out other causes of related clinical signs.
Histopathology is rarely performed in clinical practice, and biopsy is often avoided (unless there is a high level of suspicion for pancreatic neoplasia) due to cost, invasiveness, and potential for limited detection (multifocal distribution may be missed by single pancreatic biopsies).
Relevant Laboratory Tests
Routine Bloodwork
Abnormalities specific to diagnosis of chronic pancreatitis are not found on CBC, serum chemistry profile, or urinalysis; however, these tests are important for systemic evaluation of the patient, ruling out alternative differentials, and identification of concurrent disease.
Neutrophilia is common on CBC, and nonregenerative anemia of chronic disease can be seen in some cases.4
On serum chemistry profile, alterations in liver enzyme concentrations and biomarkers of kidney injury (eg, creatinine, symmetric dimethylarginine), which can be independent disease processes or secondary to chronic pancreatitis, may be seen.
Urinalysis may not reveal specific abnormalities, but proteinuria, if present, should be further quantified when appropriate via measurement of urine protein:creatinine ratio.
Abdominal Ultrasonography
Abdominal ultrasonography has a high specificity but low sensitivity for diagnosis of chronic pancreatitis; absence of ultrasonographic features of chronic pancreatitis thus does not rule out the disease.5
Ultrasonographic features vary but may include a normal to hyper- or hypoechoic pancreatic parenchyma. A heterogeneous appearance has also been suggested (Figure 1). Mass-like lesions may be noted and should not be assumed to indicate neoplasia, particularly in English cocker spaniels; in a study, ≈10% of English cocker spaniels with chronic pancreatitis had mass-like lesions.6,10
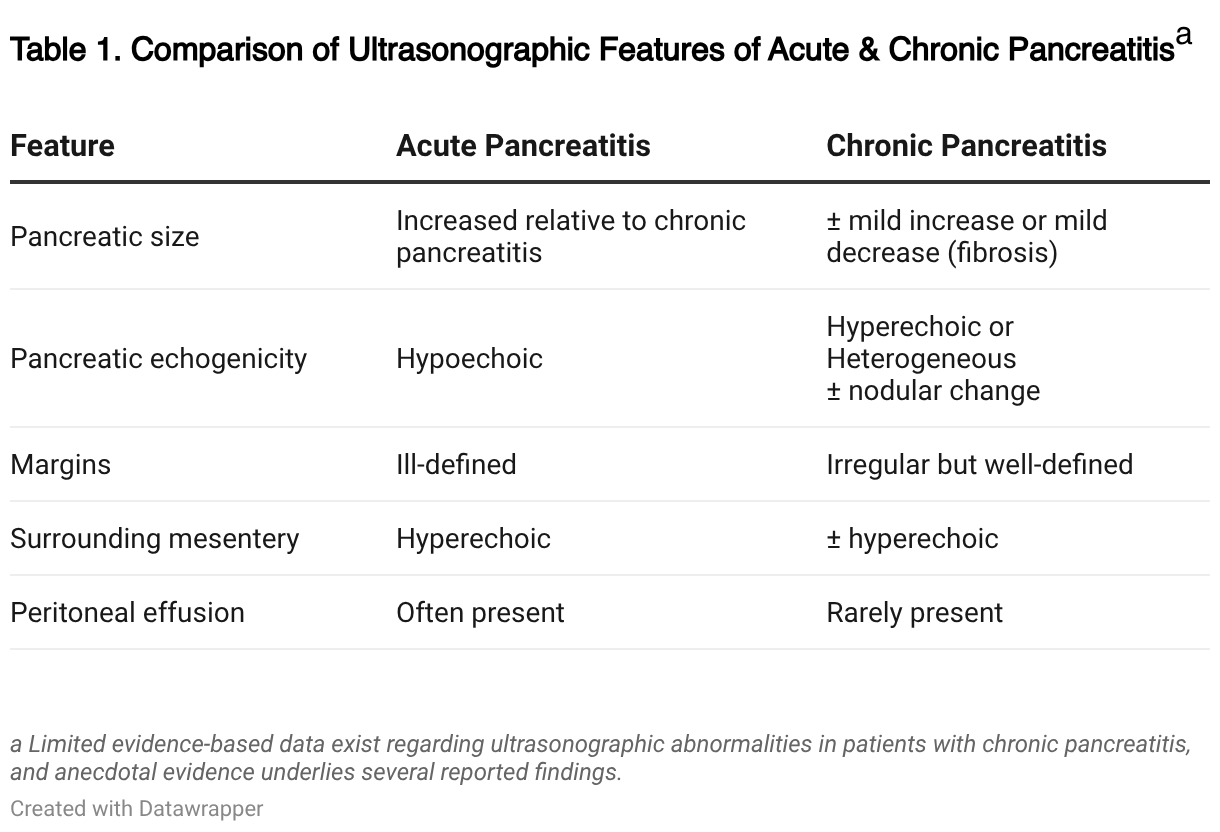
Differences between ultrasonographic features of acute and chronic pancreatitis can be seen in Table 1.
Fine-needle aspiration of the pancreas can be performed safely by trained individuals and with minimal risk for complications.11,12
Additional study is needed, and is ongoing, to investigate the degree of correlation between cytology and histopathologic findings of the pancreas.

FIGURE 1 Ultrasound images of a 12-year-old, spayed crossbreed dog showing mild enlargement (1.65 cm) of the pancreatic body, with a heterogeneous echogenicity and irregular but well-defined pancreatic borders. Clinical history and a persistent mild increase in serum pancreatic lipase concentration, without other explanation, were consistent with diagnosis of chronic pancreatitis. Acute-on-chronic disease could also have been possible.
 </noscript>
</noscript>Pancreatic Lipase
Although pancreatic lipase quantification is an important part of the diagnostic approach for suspected chronic pancreatitis, these biomarkers have a lower sensitivity for diagnosis of chronic pancreatitis relative to acute pancreatitis,13 presumably because of decreased pancreatic lipase leakage from acinar cells caused by the presence of fibrosis and loss of pancreatic mass (in the case of secondary EPI).
Even mild increases in pancreatic lipase concentration or activity may support diagnosis of chronic pancreatitis if other differentials have been ruled out.
Pancreatic lipase assays can be broadly broken down into immunologic and catalytic assays.14
Immunologic assays use antibodies targeted against specific moieties of the species-specific pancreatic lipase molecule and thus have high analytical specificity.
In contrast, catalytic assays use substrates that are broken down by pancreatic lipase (or structurally similar lipases) and thus measure enzyme activity rather than enzyme concentration.
The analytical specificity of catalytic assays appears to be dependent on both the substrate and the manufacturer.15,16
Detection of extrapancreatic lipases may make diagnosing chronic pancreatitis even more challenging and thus should be avoided when possible by selecting an analytically validated and specific assay.
Treatment
Postprandial pain is significant and likely to be initially underestimated, but behavioral changes and improvement in quality of life have been anecdotally reported after transitioning diet and administration of appropriate analgesia in dogs with chronic pancreatitis, even when overt abdominal pain was not noted at initial diagnosis.
Analgesia
Oral analgesic options are currently limited, as NSAIDs are contraindicated in the management of pancreatitis due to heightened concern for GI and renal adverse effects.13
In the United Kingdom, acetaminophen (ie, paracetamol) is often prescribed as the first-line agent to dogs without concurrent liver disease; however, this practice is currently limited in the United States, perhaps related to differences in comfort levels associated with training bias when prescribing this medication.
Acetaminophen should not be given to cats.
In the United States, gabapentin is often used in place of acetaminophen for first-line analgesic management in dogs with chronic pancreatitis.
Buprenorphine, fentanyl patches, or hospitalization may be needed if additional analgesics are used for acute-on-chronic flares of pancreatitis.
Supportive Care
Supportive care with antiemetic (eg, maropitant) and antinausea (eg, ondansetron) medications can be given as needed and combined if necessary.
Dogs may also need SC fluids if persistent dehydration is noted.
Appetite stimulants (eg, mirtazapine) can be considered on a case-by-case basis.
Nutritional Concerns
Limited research exists regarding optimal dietary management in patients with chronic pancreatitis, but a low-fat, highly digestible diet is common and may reduce postprandial pain in dogs, significantly impacting quality of life.5
Currently, no evidence suggests that adding pancreatic enzymes to the diet improves outcomes; pancreatic enzymes are therefore typically reserved only for use in patients with concurrent EPI in this population.
Treatment of Suspected Immune-Mediated Chronic Pancreatitis
Dogs with suspected IgG4-related disease should be treated supportively with topical cyclosporine for keratoconjunctivitis sicca and angiotensin-receptor blockers for proteinuria and hypertension.
If supportive treatment is not effective in controlling proteinuria or recurrent bouts of pancreatitis, consideration should be given to trial treatment with immunosuppression.
Cyclosporine or prednisone are often considered.
If possible, rare infectious etiologies should be ruled out prior to immunosuppression.
Additional studies into the effects of immunosuppression on the clinical course of chronic pancreatitis in dogs are needed.
Treatment of Secondary Complications (If Present)
Dogs with suspected chronic pancreatitis should be regularly screened for development of EPI and DM and treated based on results.
Prognosis
The long-term prognosis for chronic pancreatitis varies based on the extent of pancreatic damage and the presence of secondary complications. Early detection and intervention are critical in improving outcomes.
How Not to Overwhelm Pet Owners With Information
Avoid inundating owners with information, and help them retain key concepts with these tips.
Prepare the owner by letting them know you are about to share a lot of information.
Split information into chunks, and be strategic about what is shared when.
At the first appointment, only share information that is critical. Save noncritical information for future conversations.
Use handouts, and empathize with the owner about the amount of information to be shared.
Consider reading the handout to the owner and highlighting important information.
Provide links to helpful videos.
For more on helping owners retain education, check out this article on Avoiding Overwhelming Clients With Information.