A Novel Bandaging Method
A 5-year-old, neutered male mixed-breed dog was referred for necrotic skin resulting from bite wounds.
History. The patient had been treated for severe bite wounds (puncture wounds) over the right lateral flank one week earlier. The wounds extended over an 8 × 14 cm area but did not penetrate the abdominal muscular wall. Initial treatment consisted of copious lavage using a 0.9% saline solution and oral cephalexin.
Examination. The dog had normal vital signs and a large area of necrotic skin on the right flank region. The necrotic skin was separating from the healthy skin edges and was malodorous. Bacterial culture of exudate isolated Pseudomonas aeruginosa, which was sensitive to enrofloxacin. Initial complete blood count results revealed a mildly elevated number of white blood cells with neutrophilia. Serum chemistry profile results were unremarkable. Radiographs of the abdomen and abdominal ultrasonography revealed no evidence of penetration into the abdominal cavity.
ASK YOURSELF ...How would you initially manage this wound?A. Debride necrotic skin and apply a wet-to-dry bandage around the body.
B. Immediately debride the necrotic skin and close with a skin flap.
C. Debride the necrotic skin and apply a nonadherent dressing to the wound until a healthy granulation bed has developed; then close the wound with a skin flap.
D. Debride the necrotic skin and allow the wound to form a scab and heal by second intention.
Correct Answer: A.Debride necrotic skin and apply a wet-to-dry bandage around the body.
Treatment. In this case, a wet-to-dry bandage was placed, as the wound had been freshly debrided of necrotic material and a healthy granulation tissue bed had not developed. In addition, because of the presence of the purulent exudate, this wound needed to have open wound management to eliminate infection. The bandage was changed every 24 hours for 10 days, until healthy granulation tissue developed.
The lateral flank is very difficult to bandage, especially in a male dog, as most bandages would cover the penis. To overcome this problem, a tie-over bandage-which involves placing suture eyelets around the perimeter of the wound; then packing it with bandaging material and lacing umbilical tape through the eyelets-can be used. A tie-over bandage can be effective for small to medium wounds, or wounds that are not gravity dependent (dorsum of back). In large wounds, the sponges and packing material usually will slide ventrally, exposing the wound. Thus, tie-over is not an effective technique in such cases.
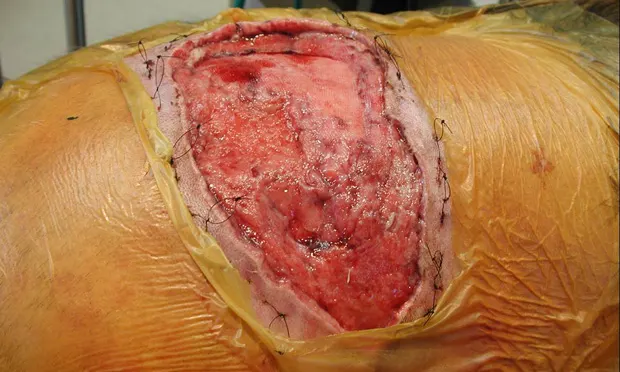
New Method: Step by Step.A novel, more effective bandaging method is the Ioban bandage (3M Health Care, www.3M.com), which is a thin, stretchy, water-repellent, antibacterial material that is sticky on one side (Figure 1). This bandage is applied in the following manner:

1. The wound is packed with large laparotomy gauze sponges (the first layer of gauze sponges may be moistened in sterile saline). The skin surrounding the wound is scrubbed with antiseptic detergent, degreased with alcohol, dried, and then liberally sprayed with an adhesive skin glue such as Vi-Drape (Medical Concepts Development, www.medconceptsdev.com).
2. The glue is allowed to dry for about one to two minutes until it has a tacky consistency; then a layer of Ioban material is applied (Figure 2).

3. To change the laparotomy sponges, a section of Ioban material is cut around the perimeter of the wound (Figure 3) with a scalpel blade, the area is packed again with sterile sponges, and a new layer of Ioban is applied to the entire area.

If the material around the wound lifts away from the skin, the Ioban bandage can be removed and reapplied as described above. Make sure that the skin is free of soap or oil residue and that the adhesive is applied liberally. If there are problems with the durability of the outer layer of Ioban, apply a second layer.

Other uses for Ioban bandages. Ioban bandages are very useful for dressing wounds located anywhere traditional bandages are difficult to apply such as the head (Figure 4), torso, and perineum. They also can be applied to the abdomen when open peritoneal drainage is implemented for the treatment of peritonitis.
An Ioban bandage can be used over the torso to prevent dehiscence of an incision that has been sutured under moderate tension following removal of a large tumor. In such a case, following closure of the incision, a thin strip of folded gauze sponges is placed over the incision line, a 4-inch area of skin on each side of the incision is liberally sprayed with Vi-Drape, and then a layer of Ioban material is applied to relieve tension from the incision. To add strength to the bandage, 4 additional layers of Ioban are then applied on top of the first layer. The Ioban is left on for about 1 week; by this time, stress relaxation of the collagen fibers has occurred and the natural incisional tension has greatly decreased. If it is difficult to remove the Ioban, it can be left to exfoliate with the skin. Keep in mind that this tension-relieving technique should not be relied on to compensate for poor surgical technique. This technique is also not appropriate on limbs as it could potentially compromise perfusion to the extremities.
Discussion. Ioban is frequently used in both human and veterinary surgery to reduce skin-related contamination during orthopedic and soft tissue surgery. It is economical, as it requires much less material than a traditional bandage wrapped around the body. In addition, Ioban takes much less time to apply than a traditional bandage. It also maintains a moist environment of the wound as it is occlusive, which has been shown to be beneficial to healing skin wounds. The days of allowing wounds to dry out and form a protective scab have gone by the wayside. Current research shows that a moist, warm environment actually promotes healing by hastening granulation tissue formation and epithelialization.
Keys to success. The correct timing and application of appropriate bandage techniques are keys to successful wound management. Absorbent, debriding bandages such as a wet-to-dry bandage should only be used when there is tissue that needs to be eliminated or discharge that needs to be removed from the wound. Once granulation tissue has formed, bandages that stick to wounds will damage healthy tissue that is starting to form, thus they must not be used. A nonadherent contact layer such as Telfa or Adaptic (Tyco Healthcare, www.tycohealthcare.com), may be beneficial at this time if a granulation bed is needed prior to skin wound reconstruction with a graft or flap, or if second intention healing is the goal.
THE ANSWER EXPLAINED ...Infected and necrotic wounds must be managed prior to primary surgical closure and several days of appropriate bandage care can make a huge difference in the success of any delayed surgical repair.
Bandages that encompass the chest and abdomen are difficult to apply and maintain. They frequently slip cranially or caudally and expose the wound.
Tie-over bandages are useful in difficult areas of the body; however, they are not useful for large wounds.
An adherent primary-contact layer of bandage (wet-to-dry) debrides the wound and effectively removes exudates in the early phases of healing.
A nonadherent primary-contact layer of bandage is used once a healthy bed of granulation tissue has developed, when additional time is needed prior to the primary repair, or when second intention healing is desired.
TAKE-HOME MESSAGES
Proper bandage care is vital to the treatment of large open wounds. Multiple bandaging techniques may be required to help serious wounds heal successfully.
Novel use of adherent, sterile materials such as Ioban can greatly enhance cleanliness and ease of bandaging with multiple applications.
Ioban materials can be used to relieve tension of tight incisions and for the application of absorbent, protective, or debriding bandages in difficult locations.
A NOVEL BANDAGING METHOD • Susan C. Hodge & Daniel Degner
Resources
Vi-Drape, Medical Concepts Development, Woodbury, MinnesotaPhone: 800-533-3974www.medconceptsdev.comIoban 2, 3M Health Care, St Paul, MinnesotaPhone: 800-228-3957www.3M.comTelfa and Adaptics, Tyco Healthcare, Mansfield, MassachusettsPhone: 800-962-9888www.tycohealthcare.com