Noncutaneous Adverse Drug Reactions - Part 1
Part 1: HepatotoxicityThis review is the first of a 2-part series. It will focus on dose-dependent and idiosyncratic drug reactions in the liver in dogs and cats; part 2 will discuss adverse drug reactions affecting the blood cells and bone marrow.
Types of Reactions Adverse drug reactions can be categorized as dose-dependent or idiosyncratic, although there is some overlap between the two.
Dose-Dependent Reactions For dose-dependent reactions, toxicity increases as the dose increases in a particular species, and virtually all members of a population are affected at high enough dosages. Dose-dependent reactions may be caused by the drug itself or by a consistently generated metabolite. These reactions can be related to the desired pharmacologic action of the drug (eg, bradycardia from diltiazem), or can be unrelated to the desired effect (eg, retinal toxicity from fluoroquinolones).
Dose-dependent reactions are relatively predictable, and therapeutic drug monitoring (eg, measuring serum digoxin concentrations) may be helpful to determine when such reactions might occur. Dose-dependent reactions require a dose reduction, but usually not drug avoidance.
Idiosyncratic Reactions Idiosyncratic drug reactions lead to toxicity at therapeutic doses in a small proportion of patients. Toxicity does not increase with dose in the general population, but probably does increase with dose in susceptible individuals. Idiosyncratic reactions are by definition unpredictable, and therapeutic drug monitoring is generally not helpful. These reactions are usually not related to the desired pharmacologic action of the drug, and are believed to arise most commonly from variable metabolism of the drug in certain individuals. Although idiosyncratic drug reactions are also called "drug hypersensitivity reactions," they may or may not involve an immunologic response.
Signs of idiosyncratic adverse drug reactions most commonly occur within the first 2 to 3 weeks of therapy, but can arise later in treatment. They almost always require discontinuation of the suspect drug. Structurally related drugs may cause a similar reaction. Common targets of idiosyncratic drug toxicity are the skin, liver, and bone marrow; the eyes and the central nervous system are less commonly affected.
Related Article: Cutaneous Adverse Drug Reactions

Hepatotoxicity The liver is particularly susceptible to drug toxicity because it is the site of first-pass clearance of many orally administered drugs and of P450-mediated bioactivation of compounds to more reactive metabolites. Acute drug-induced hepatotoxicity, either dose-dependent or idiosyncratic, typically has a predominant cholestatic or cytotoxic (ie, hepatic necrosis) pattern. Both can result in jaundice (Figure 1), although reactions involving cholestasis alone tend to be less severe.
Figure 1. Drugs can lead to hepatotoxicity with jaundice, either due to massive hepatic necrosis or drug-induced cholestasis.
Dose-Dependent Reactions Affecting the LiverAcetaminophen

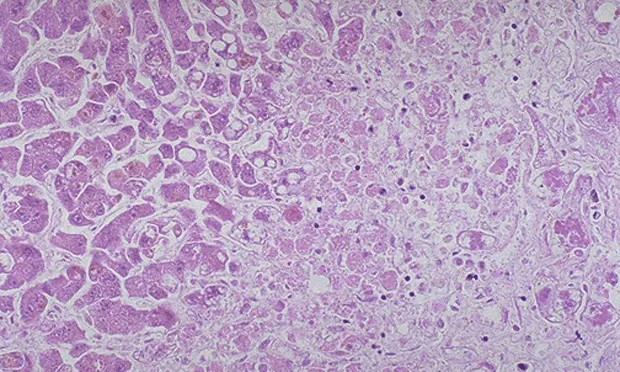
Acetaminophen administration in both dogs and cats leads to dose-dependent acute centrilobular hepatic necrosis (Figure 2). Dogs have similar susceptibility to acetaminophen toxicity as humans, with a toxic dose of 150 to 250 mg/kg. Acetaminophen is bioactivated to an oxidized metabolite by CYP2E1, a cytochrome P450 that is induced by phenobarbital; this reactive metabolite is detoxified by glutathione conjugation. Phenobarbital administration and glutathione depletion could therefore increase the risk for acetaminophen toxicity in dogs.
Figure 2. Liver necrosis caused by acetaminophen. Courtesy Sharon Gwaltney-Brant, ASPCA Animal Poison Control Center
The unique susceptibility of cats to doses of acetaminophen that are safe in humans and dogs can be attributed to an acetaminophen glucuronidation pathway in cats that is more than 30-fold less efficient than that in dogs.1 Specific therapy for acetaminophen hepatotoxicosis includes the glutathione precursor N-acetyl-cysteine (NAC) or, alternatively, S-adenosylmethionine (SAMe) in patients that are less severely affected and can tolerate oral medications.
Itraconazole & Ketoconazole In dogs and cats, there are clinical reports of increased ALT, with or without cholestasis, associated with itraconazole and ketoconazole. In dogs, increases in serum ALT and ALP correlate with serum itraconazole concentrations,2 and these enzyme elevations resolve with drug dose reduction. In humans, ketoconazole hepatotoxicity appears to be due to an oxidative metabolite, without evidence of an immune reaction. Hepatotoxicity from fluconazole or itraconazole appears to be less common than that from ketoconazole.
Azathioprine Azathioprine can also lead to mild to marked increases in ALT in dogs. Glutathione depletion is a likely contributor in experimental models. Dogs treated with azathioprine should have ALT monitored at each recheck; if an otherwise-unexplained increase in ALT is noted, azathioprine should be discontinued temporarily and restarted at a lower dose, with careful monitoring of ALT and clinical status.
Phenobarbital Phenobarbital leads to liver enzyme induction (serum ALP and GGT) in dogs, which may progress to hypoalbuminemia, increases in bile acids, and overt cirrhosis.3 Possible mechanisms of toxicity include depletion of antioxidants or essential cofactors, or induction of cytochrome P450 enzymes with secondary bioactivation and toxicity of other substances (drugs, dietary components, environmental toxins). A direct cytotoxic effect is unlikely, since hepatotoxicity is not seen with loading doses. Prolonged duration and high doses appear to be risk factors, as is prior therapy with either primidone or phenytoin.
If phenobarbital hepatotoxicity is suspected, the drug should be discontinued or the dose substantially reduced. A loading dose of KBr (400 to 600 mg/kg divided over 4 doses) can be given if immediate phenobarbital discontinuation is desired; otherwise, KBr may be started at a maintenance dose of 40 to 60 mg/kg/day, with a rapid taper of phenobarbital over 2 to 4 weeks. Early detection of phenobarbital hepatotoxicity can be achieved by screening treated dogs with serum bile acids every 6 to 12 months, and monitoring for hypoalbuminemia, increased bilirubin, clinical illness, or increased sedation.
In contrast to dogs, cats are not affected by phenobarbital hepatotoxicity, and liver enzyme induction is not seen. The reason for this difference is not known.
Idiosyncratic Reactions Sulfonamides Potentiated sulfonamide antimicrobials can lead to hepatocellular necrosis, cholestasis, or both in dogs.4 These reactions are believed to be due to an oxidized metabolite that covalently binds to proteins and acts as a hapten. The delay in onset from drug exposure to adverse reaction of 7 to 14 days suggests an immune mechanism, and we have documented antidrug antibodies in dogs with sulfonamide toxicity.5 All dogs treated with potentiated sulfonamides should have careful clinical monitoring for inappetence, lethargy, vomiting, or darkened urine. Prompt drug discontinuation can be lifesaving. Although not clinically evaluated, supportive care including antioxidant supplementation with ascorbate (90 mg/kg/day) and NAC may be beneficial.

Diazepam On rare occasions diazepam leads to fulminant hepatic necrosis in cats (Figure 3), with marked increases in ALT as well as jaundice and encephalopathy.6 The delay of 8 to 9 days from exposure to onset of signs (reported initially) suggests an immune pathogenesis, but some cats show signs of toxicity within 96 hours of first exposure. There are no known breed predilections, and cats with no underlying disorders other than behavioral problems have been affected. Diazepam hepatotoxicity requires aggressive supportive care for liver failure, including administration of intravenous fluids and plasma, vitamin K1, gastric antacids, antimicrobial coverage for bacterial translocation, lactulose, and nutritional support. Diazepam hepatoxicity has not been reported with injectable diazepam or midazolam.
Figure 3. Liver necrosis caused by diazepam. Courtesy Sharon Gwaltney-Brant, ASPCA Animal Poison Control Center.
Carprofen On rare occasions carprofen can lead to acute hepatic necrosis in dogs; toxicity is characterized by marked increases in ALT and jaundice due to hepatic failure.7 Most dogs become affected 14 to 30 days after drug initiation. Although Labrador retrievers were overrepresented in an initial report, the manufacturer of carprofen has not been able to reproduce this syndrome in Labradors under controlled conditions. The reported incidence is 1.4 cases per 10,000 dogs treated (< 0.02%). Because of the acute onset and rarity of this reaction, routine biochemical monitoring of ALT in clinically normal dogs is probably not warranted. Clinical monitoring is key, with owners instructed to watch for any signs of lethargy, inappetence, vomiting, or diarrhea. Clinically ill dogs, even if only mildly affected, should be immediately evaluated for increases in ALT, as well as for more common side effects, such as gastric ulceration or renal decompensation. Increases in serum ALP without higher increases in ALT are unlikely to be caused by carprofen.
Methimazole Methimazole leads to hepatotoxicity in about 2% of cats, with either a cytotoxic pattern (increased ALT) or cholestatic pattern (increased serum ALP and bilirubin).8 In humans, liver toxicity from methimazole has been attributed to an oxidized metabolite generated in the liver, and glutathione depletion enhances methimazole hepatotoxicity experimentally. It is important to distinguish increases in ALT due to hyperthyroidism from methimazole-induced increases in ALT. ALT should fall, not rise, during methimazole treatment, as serum T4 normalizes.
For cats that become ill during methimazole treatment, a minimum database should include a CBC to rule out blood dyscrasias; BUN and creatinine to rule out renal decompensation; and ALT, serum ALP, and bilirubin to rule out hepatotoxicity. If blood analysis results are normal, inappetence and vomiting may be due to simple gastrointestinal upset, which should respond to a dose reduction or change to transdermal methimazole. Transdermal methimazole is not appropriate in cats with hepatotoxicity from oral methimazole.9 If liver enzymes are rising, methimazole should be discontinued and radioiodine should be scheduled.
Glipizide Glipizide can cause cholestatic jaundice and increases in serum ALP in about 8% of diabetic cats.10 These changes resolve with drug discontinuation. Glyburide, another sulfonylurea hypoglycemic agent, inhibits bile acid efflux through biliary transporters, leading to cholestasis in humans. The two drugs share structural similarities, making this a likely mechanism for glipizide as well.
ALT = alanine transaminase; ALP = alkaline phosphatase; BUN = blood urea nitrogen; CBC = complete blood count; GGT = gamma-glutamyl transferase; KBr = potassium bromide; NAC = N-acetyl-cysteine; SAMe = S-adenosylmethionine