Neurogenic Keratoconjunctivitis Sicca in Dogs
Ursula M. Dietrich, DVM, DACVO, DECVO, FHEA, The London Cat Clinic, London, United Kingdom
In the Literature
Galley AP, Beltran E, Pont RT. Neurogenic keratoconjunctivitis sicca in 34 dogs: a case series. Vet Ophthalmol. 2022;25(2):140-152. doi:10.1111/vop.12949
The Research ...
Quantitative keratoconjunctivitis sicca (KCS), a deficiency of the aqueous portion of the precorneal tear film, is common in dogs. Possible neurogenic causes are not often recognized or considered.
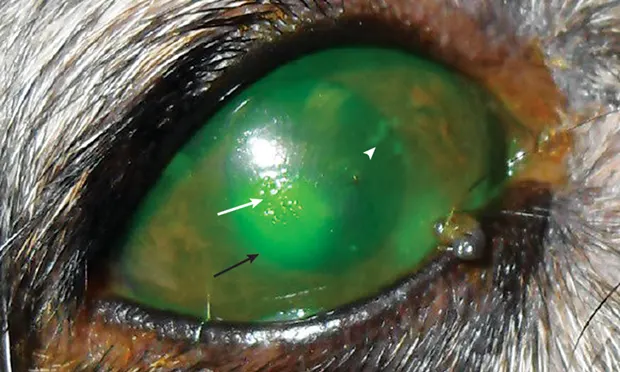
Lacrimal and nictitans glands, lateral and mucosal nasal glands, and palatine glands are innervated by postganglionic parasympathetic fibers of the facial nerve. Damage or trauma to these fibers may lead to neurogenic KCS, which causes typical clinical signs of KCS (eg, mucopurulent ocular discharge, blepharospasm, conjunctival hyperemia, corneal neovascularization or ulceration). The ipsilateral nostril is typically dry and crusty (ie, xeromycteria), indicating decreased function of mucosal nasal glands.
This retrospective study analyzed ocular and neurologic signs, diagnostic imaging findings, underlying conditions, and response to treatment in 34 dogs with neurogenic KCS. Ocular signs of KCS were present in all dogs, and neurologic signs (eg, facial neuropathy, peripheral vestibular syndrome, Horner syndrome) were identified in 52.9% of dogs. MRI or CT was performed to further investigate neurologic signs in 18 dogs. Based on patient history, clinical signs, and available imaging findings, suspected etiologies for neurogenic KCS included chronic otitis interna/media, iatrogenic facial nerve damage after total ear canal ablation and lateral bulla osteotomy, head trauma, brainstem tumor, and an area of inflammation in the pterygopalatine fossa.
Treatment was administered to 30 dogs. Response to a lacrimostimulant (cyclosporine 0.2% or tacrolimus 0.05%) alone was poor in the 4- to 10-month treatment period. Oral pilocarpine 2% with or without a lacrimostimulant, however, led to improved clinical signs, improved Schirmer tear test results, and resolution of xeromycteria in 48% of the 23 dogs available for follow-up.
... The Takeaways
Key pearls to put into practice:
Neurogenic KCS is caused by damage to the preganglionic parasympathetic fibers of the facial nerve that innervate the ocular tear glands, mucosal nasal glands, and palatine glands. In addition to typical signs of KCS, affected dogs may exhibit ipsilateral xeromycteria and neurologic signs.
Results from this study suggest neurogenic KCS is common in older (>8 years of age) dogs, small dogs, and crossbreed dogs, with a potential breed predisposition in English cocker spaniels and Cavalier King Charles spaniels. Underlying endocrinopathy (eg, hypothyroidism, diabetes mellitus) may also predispose patients to peripheral neuropathies and subsequent neurogenic KCS. Advanced imaging (eg, CT, MRI) may help investigate the underlying cause of neurogenic KCS, but the condition is often idiopathic.
Oral pilocarpine is the treatment of choice for neurogenic KCS and is preferable in combination with a lacrimostimulant (ie, cylosporine, tacrolimus). The ophthalmic preparation of pilocarpine 2% is initially administered at 1 drop/10 kg (0.1 drop/kg) PO every 12 to 24 hours with food, increased by 1 drop every 1 to 3 days until systemic adverse effects (eg, hypersalivation, vomiting, diarrhea) are noted, then decreased to the previous dose for maintenance.
You are reading 2-Minute Takeaways, a research summary resource presented by Clinician’s Brief. Clinician’s Brief does not conduct primary research.