This response is correct!
Meniscal Disease
Mary Sarah Bergh, DVM, MS, DACVS, DACVSMR, Midwest Veterinary Specialists, Milwaukee, Wisconsin
The medial and lateral menisci are fibrocartilaginous structures in the stifle joint that play an important role in normal joint function. The menisci distribute load, improve congruity, enhance stability, provide proprioceptive functions, and provide lubrication to the articular cartilage.1-4 The menisci have poor blood supply—only the peripheral 25% is supplied blood by the medial and lateral genicular arteries—leading to poor healing of meniscal disease and impacting the clinical significance and treatment of meniscal tears.1,3,5,6
Background & Pathophysiology
Meniscal injury in dogs and cats primarily occurs secondary to stifle instability resulting from cranial cruciate ligament (CCL) rupture.7-18 Isolated meniscal tears are rare and may be more likely to occur secondary to trauma or in canine athletes; a limited number of these cases have been reported.8,10-12 CCL rupture is the most common cause of pelvic limb lameness in dogs, and ≥85% of dogs—and 67% of cats—with CCL rupture have been reported to have meniscal tears diagnosed at the time of surgery.12,13 Postoperatively, meniscal tears can also occur secondary to persistent stifle instability and have been reported in 0.7% to 27.8% of dogs, with the lowest rates generally following tibial plateau leveling osteotomy (TPLO) surgery and the highest rates generally following tibial tuberosity advancement surgery.15-18
Spayed/neutered, older, and obese dogs, as well as certain breeds (eg, rottweilers, Newfoundlands, Staffordshire terriers), have been shown to have a higher risk for CCL rupture.19,20 Specific risk factors for the development of meniscal tears after CCL rupture include increased stifle instability, increased duration of lameness, increased weight, and older age.21-23
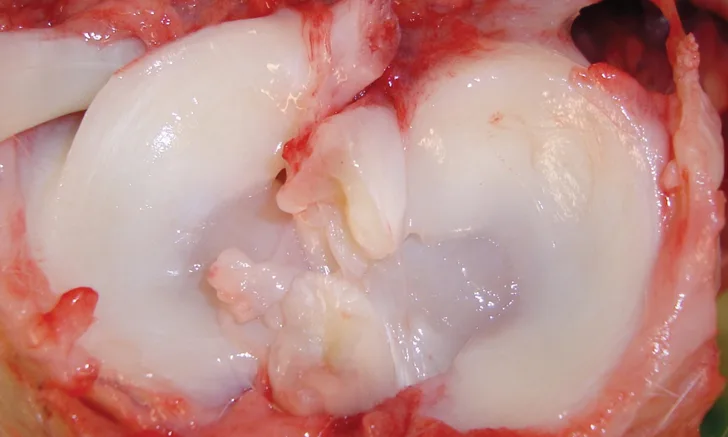
Although there are 2 menisci in the stifle joint, >96% of meniscal tears occur in the medial meniscus alone.1,2,4,13,15,16,24 This is secondary to anatomic differences between the medial and lateral menisci. Both menisci are attached cranially to the tibia, but the medial meniscus is more closely associated with the tibial plateau because of its firm attachment at the medial collateral ligament, peripheral attachment to the joint capsule, and primary caudal attachment to the tibia at the meniscotibial ligament. The lateral meniscus lacks an attachment at the collateral ligament, has looser capsular attachments, and has its primary caudal attachment on the femur versus the tibia. When the CCL is ruptured (Figure 1), the femoral condyles translate caudally during weight-bearing, leading the lateral meniscus to translate caudally with the lateral femoral condyle. The medial meniscus, which is more firmly attached to the tibia, is then crushed by the medial femoral condyle when it translates caudally. Excessive rotational forces in the stifle, either from CCL rupture or supraphysiologic loads, can also lead to meniscal injury.8,25,26 Tears may be partial or full thickness through the meniscus.
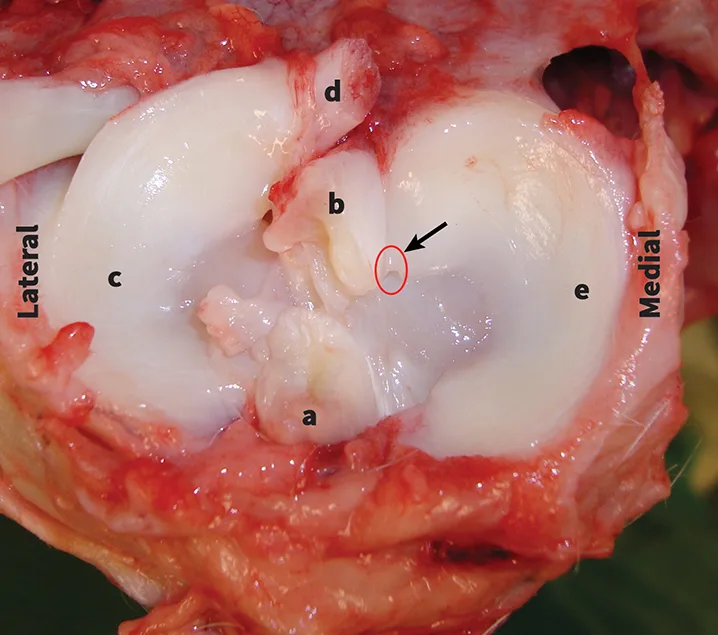
Anatomic specimen of a disarticulated stifle that demonstrates the meniscal anatomy: CCL (a), caudal cruciate ligament (b), lateral meniscus (c), caudal meniscofemoral ligament (d), medial meniscus (e), caudal meniscotibial ligament (arrow)
The caudal pole region between the medial collateral and meniscotibial ligaments is the most commonly injured portion of the medial meniscus. Common configurations include vertical longitudinal (ie, bucket handle) tears, maceration of the caudal pole, peripheral capsular detachment, and radial tears. The most clinically relevant tears are medial meniscal; however, 77% of arthroscopically evaluated dogs with CCL rupture had some degree of damage to the lateral meniscus.24,25,27 Lateral meniscal tears tend to be radial or longitudinal and, although the clinical significance is unclear, a recent report found significant cartilage lesions associated with isolated lateral meniscal tears in dogs, suggesting that there is a negative impact on joint health.12,24
History & Clinical Signs
Dogs and cats with meniscal tears are typically presented with chronic or acute pelvic limb lameness that is often only partially alleviated with conservative management (including NSAIDs and rest); CCL rupture may or may not have been previously diagnosed, and stifle surgery for CCL rupture may have been previously performed.10,11,24,28-30 Development of a meniscal tear is typically associated with sudden worsening of lameness in patients that were previously diagnosed with CCL rupture or a new onset of lameness in dogs that have previously undergone surgery for CCL rupture.17,18,24 The presenting lameness is often more severe in dogs that have CCL rupture and meniscal tears as compared with dogs that have only CCL rupture; it is not uncommon for this to be nonweight-bearing lameness.22,23 Some owners report hearing a popping or clicking sound when their pet is ambulating. Meniscal injury should be a differential diagnosis for dogs that have had stifle surgery for CCL rupture and are presented with subtle or acute profound lameness or have poor clinical recovery after surgery.15,16,22,24,30
Because meniscal disease primarily occurs in conjunction with CCL rupture, clinical findings support both conditions. Orthopedic examination often reveals partial to nonweight-bearing pelvic limb lameness and variable amounts of musculature atrophy on the affected pelvic limb.8-11,22,23 Palpation of the stifle joint can reveal periarticular thickening and palpable joint effusion.9,11,18 Stifle range of motion may be decreased secondary to pain or periarticular fibrosis in the case of chronic disease. Pain with flexion of the stifle joint is an indicator of meniscal injury in some cases.11,23 Approximately 28% to 38% of dogs with meniscal injury have an audible popping sound (ie, meniscal click) during flexion and extension of the stifle that occurs when the medial femoral condyle slides up and over the caudal pole of the medial meniscus.8,23,24,31 Dogs with meniscal tears are often positive for cranial drawer motion and tibial thrust secondary to CCL rupture.
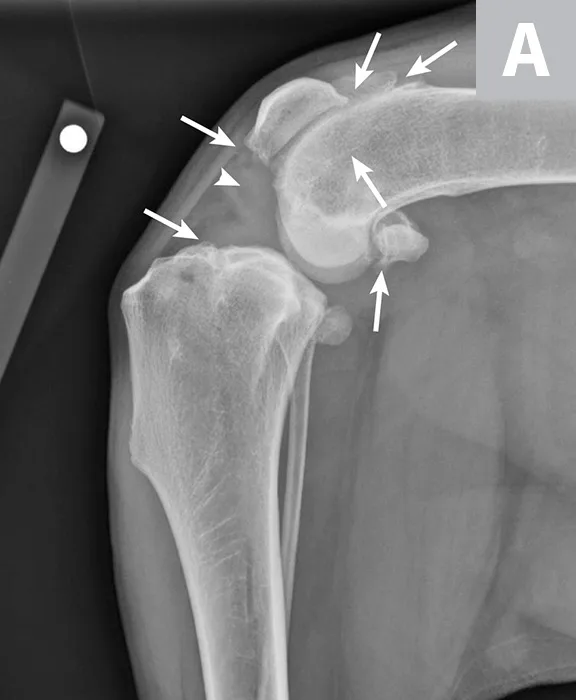
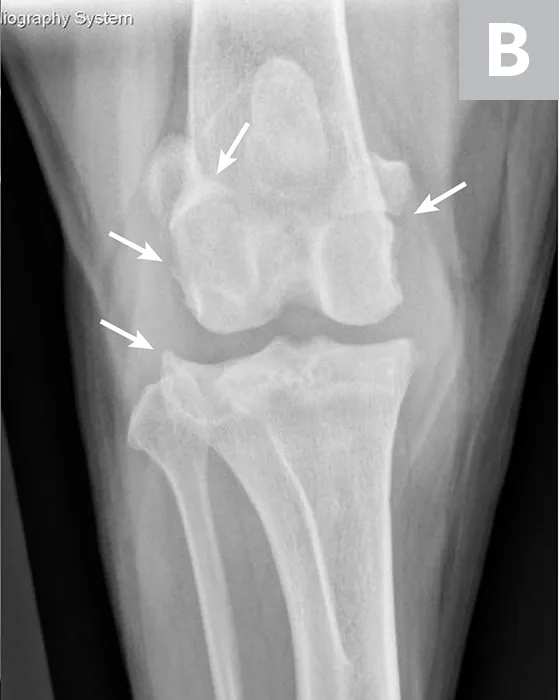
Mediolateral (A) and craniocaudal (B) radiograph projections of a 3-year-old spayed mastiff with right CCL rupture and medial meniscal tear. Osteophytes are present on the femoral condyles, patella, fabellae, and tibial plateau (arrows). There is increased soft tissue opacity in the joint space consistent with joint effusion (arrowhead). In addition, there is cranial displacement of the tibia relative to the femur on the lateral projection. These signs combined are consistent with CCL rupture.
Diagnosis
Clinical history and orthopedic examination are key to diagnosing meniscal injury, but diagnosis cannot be confirmed using only these methods. Orthogonal radiography of the affected stifle joint can be used to evaluate the presence and severity of osteoarthritis and can help rule out other pathologies (eg, osteochondritis dissecans, fracture, neoplasia) of the stifle. In dogs with CCL rupture and possible meniscal injury, osteophytosis, increased soft tissue opacity in the joint space (ie, joint effusion), and increased soft tissue opacity on the medial aspect of the joint (ie, medial buttress) are commonly seen on radiographs (Figure 2); however, it is possible to see little to no osteoarthritis in acute injuries. The meniscus cannot be directly visualized on radiographs and identification of meniscal tears is limited, even with computed tomography arthrography.32,33 A skilled ultrasonographer may be able to identify some tears in the meniscus34-37; however, MRI is a more readily available and reliable, noninvasive method to evaluate the presence of meniscal tears.37-40
Surgical exploration of the stifle joint is typically used to identify tears in the meniscus. The most accurate method for diagnosing a meniscal tear is joint evaluation by arthroscopy or arthrotomy, combining visual evaluation and careful palpation of the meniscus with a meniscal probe.41 A stifle distractor or Hohmann retractor may be necessary to facilitate adequate access to inspect the caudal portions of the joint (Figure 3). Both menisci should be carefully evaluated to identify all damaged regions.41 Failure to identify and treat meniscal tears is a common cause of poor function following surgery for CCL rupture.24,30,41,42
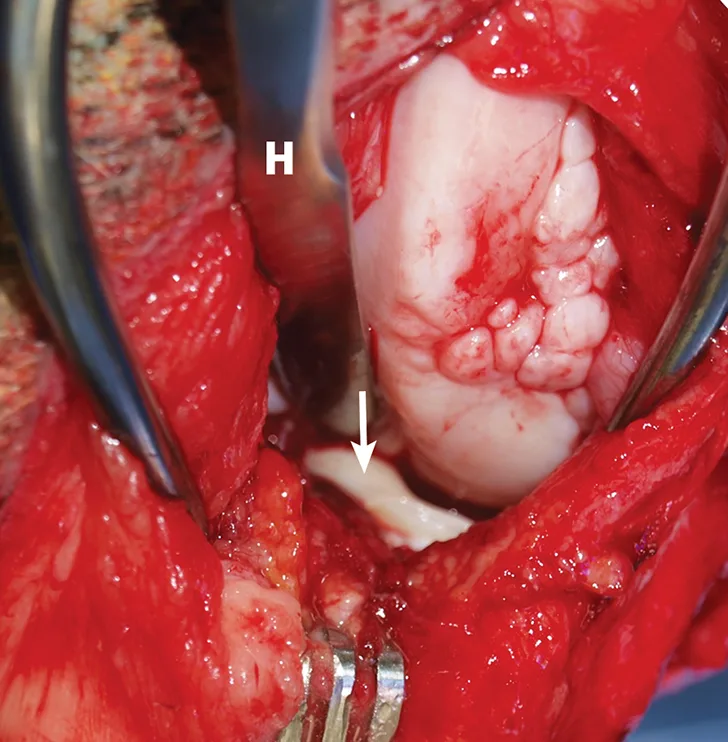
Intraoperative image demonstrating identification of medial meniscal tears by craniomedial arthrotomy in the dog in Figure 2. A Hohmann retractor (H) has been placed to allow inspection of the caudal joint space. The caudal pole of the medial meniscus has sustained a bucket handle tear and is flipped cranially (arrow).
Treatment & Management
Because there is poor blood supply to the menisci, meniscal tears are unlikely to heal on their own, and surgery should be the primary treatment. Surgical treatment usually involves removing the torn portion of the meniscus; however, it may be possible to repair specific meniscal tears located in the outer 25% of the meniscus where the blood supply is better.14 Better success with meniscal repair or regeneration in dogs and cats is possible in the future.42,43
Treatment for meniscal tears depends on the tear location and severity.14,24,28-30 If the entire caudal pole is damaged, it should be removed via caudal pole hemi-meniscectomy.44 If only the inner rim of the caudal pole is damaged, a partial meniscectomy (ie, removal of the damaged inner rim), leaving the periphery intact and possibly preserving some of the function of the meniscus (Figure 4), can be performed. The normal meniscus is generally left in situ.
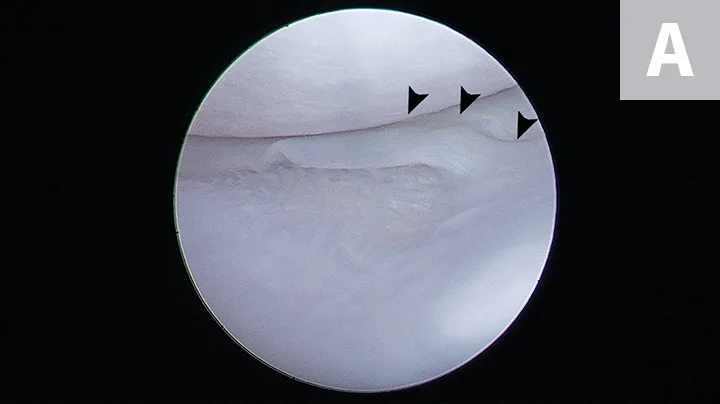
FIGURE 4A
Arthroscopic images showing a small bucket handle tear in the caudal pole of the medial meniscus (A; arrowheads). The meniscus is palpated with a meniscal probe (B; P). The torn portion of meniscus is removed with an arthroscopic shaver (C; S). After removal of the diseased meniscus, the remaining outer rim of the meniscus is left intact (D).
If there is instability of the stifle secondary to CCL rupture, surgery to stabilize the stifle is indicated following treatment of the meniscal tear. Common methods of stabilizing a CCL-deficient stifle include TPLO, lateral fabellotibial suture, and tibial tuberosity advancement. The potential risks and benefits of performing a meniscal release—in which the medial meniscus is transected to allow more movement of the meniscus—are debated. This procedure can reduce, but not eliminate, the chance of meniscal tears postoperatively; however, it changes the contact mechanics in the stifle joint, subsequently reducing stability and causing osteoarthritis.41,45,46 Physical rehabilitation can improve the speed and extent of recovery postoperatively and may have long-term benefits.47,48
Because dogs and cats can develop progressive osteoarthritis and decreased stifle range of motion secondary to meniscal injury, ongoing medical therapy with weight management, joint supplements, physical rehabilitation therapy, and pain medication may be needed.12,49,50 After TPLO surgery, dogs fed a protein-rich omega-3 fatty acid diet were shown to have increased limb use as compared with dogs fed a standard adult diet.51
Prognosis
Surgical removal of the torn meniscus often results in rapid resolution of pain and lameness.11,15,24,28,29 The long-term functional outcome can be variable depending on the preoperative disease state of the joint and the surgical procedure performed to address the concurrent CCL disease, if applicable. TPLO currently has the best evidence supporting the ability of dogs to consistently return to normal clinical function and the lowest reported rate of postoperative meniscal tears.17,52 Although removing the torn meniscus can change biomechanics in the stifle joint and cause osteoarthritis, a difference has not been seen in the functional outcome between dogs with TPLO treated with and without meniscectomy for CCL rupture.28,29
Conclusion
Meniscal tears are common in dogs and cats with CCL rupture and can occur rarely as isolated events. Incidence increases with increased stifle laxity and chronicity of CCL rupture. Radiography and orthopedic examinations alone are not sensitive enough to diagnose meniscal injury. MRI or surgical joint exploration using arthroscopy or arthrotomy with meniscal probing can confirm diagnosis. Meniscal tears are commonly treated with surgical debridement; concurrent surgical stabilization of the CCL-deficient stifle is advised. Although the postoperative outcome for meniscal injury is typically good, stifle osteoarthritis may require ongoing management.