Hypertension
Hypertension in small animal patients is generally secondary to an underlying disease process. In some older cats, an underlying reason cannot be found, even with a thorough workup. This is probably best referred to as idiopathic hypertension, rather than primary or essential hypertension, the terms commonly used when referring to nonsecondary hypertension in humans.
Hypertension should be suspected whenever a small animal patient has a disease known to cause increased blood pressure, such as renal disease (renal failure, glomerulopathy), hyperadrenocorticism, adrenal tumor, and hyperthyroidism. Hypertension should also be considered when clinical signs suggesting target organ damage are present, including:
Ocular changes (retinal hemorrhage/detachment, hyphema, acute blindness, retinal vessel tortuosity or perivascular edema, papilledema, and glaucoma)
Cardiac changes (left ventricular hyper-trophy, murmurs, gallop rhythm, and arrhythmia)
CNS signs (depression, stupor, seizures) or any neurologic sign.
Defining hypertension can be challenging, given the various technologies available to measure blood pressure and the difficulties associated with accurate and reproducible blood pressure measurement in small animal patients. The Table shows guidelines based upon the ACVIM consensus statement on identification, evaluation, and management of hypertension in dogs and cats. The stratification of hypertension is based on the risk for target organ damage.
Measuring Blood Pressure
When diagnosing hypertension, it is obviously crucial that blood pressure readings are accurate. A hospital protocol should be established to ensure consistent technique. Minimizing stress is vital (Figure 1). Various technologies, each with their own pros and cons, are available (see Devices: Blood Pressure Monitors, September 2005, available at www.cliniciansbrief.com). Staff must familiarize themselves with the equipment and become comfortable in its use.
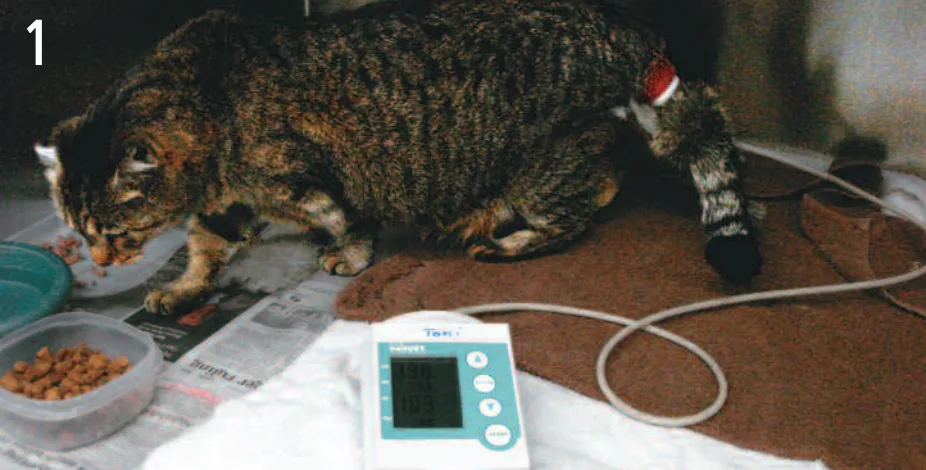
Measuring blood pressure with an oscillometric device. The cat does not seemed to be stressed during this procedure; it is eating while the measurements are being taken.
In some cases, getting any reading can be extremely difficult-for example, in stressed or fractious animals. However, recent technologic advances such as high-definition oscillometry (HDO) (Memo Diagnostic; S+B MedVet, www.submedvet.com) have made it possible to obtain oscillometric readings relatively easily on the tail of cats and dogs, to the point where owners can accomplish this themselves. The equipment also stores a downloadable oscillometric trace for manual evaluation, allowing the clinician to determine whether a relatively artifact-free tracing was obtained or if it was predominantly erroneous (Figures 2 and 3).
Table: Classification of Hypertension Based on the Risk for Target Organ Damage
ACVIM = American College of Veterinary Internal Medicine
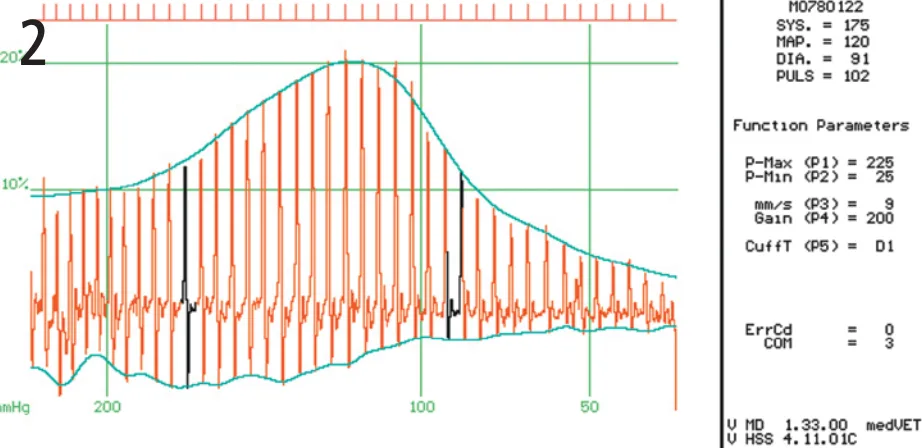
High-definition oscillometry (HDO) tracing from a dog. This is a good tracing, with near normal distribution and few artifacts. The blood pressure readings obtained can be seen on the right-hand side.
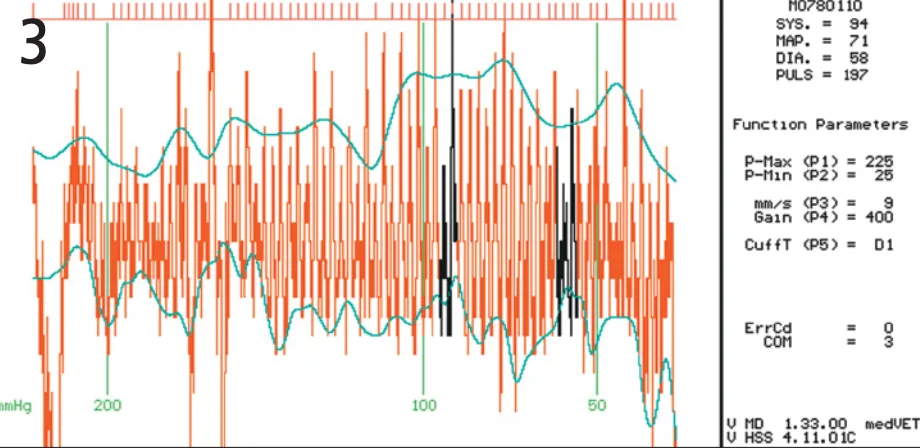
HDO tracing showing considerable artifacts. In this case, the readings are unreliable.
Target Organ Damage
Ocular
Hypertension can damage a variety of organs; however, the eyes are especially susceptible to injury. Hypertension can cause retinopathy, choroidopathy, and/or optic neuropathy (Figure 4). It can also result in hyphema or hemorrhage, including intravitreal, in some patients. It should be considered as a potential cause of other ocular problems, such as glaucoma. Screening the retinas, in most cases with indirect ophthalmoscopy, of all patients with diseases that can cause hypertension, in confirmed hypertensive patients, and in geriatric patients-especially cats-is good policy.

Bullous retinal detachment in a hypertensive cat. This occurs most consistently with choroidopathy.
Renal
Hypertension commonly causes damage to the kidneys and is a major cause of chronic end-stage renal disease in humans. In small animal patients, clinically relevant damage to the kidneys is usually seen only in patients with preexisting renal disease; of course, this tends to be relatively common since renal disease is the most common cause of hypertension in small animal patients. This becomes a vicious cycle-kidney disease causes hypertension and hypertension worsens the kidney disease. In these patients, kidney disease has resulted in loss of autoregulation, which is the ability of the renal vasculature to buffer the effects of both hypotension and hypertension on renal and glomerular perfusion.
Cardiac
Hypertension causes cardiac changes. High blood pressure increases afterload, which causes a compensatory increase in cardiac wall thickness (concentric left ventricular hypertrophy). This change compensates for increased afterload but causes reduced diastolic pressure. Unlike cats with hypertrophic cardiomyopathy, however, patients with hypertension generally exhibit a preserved internal diameter of the left ventricle. Common clinical findings in hypertensive patients include gallop rhythms, murmurs, arrhythmias, and tall R waves on electrocardiography.
Central Nervous System
CNS signs are the most severe complication of hypertension. Autoregulation of CNS blood vessels is used to reduce the effects of high blood pressure and over time this leads to vascular changes that can result in ischemia and/or hemorrhage as well as edema, which can increase intracranial pressure. There are several clinical manifestations, including depression, lethargy, circling, seizures, cranial nerve deficits, and coma. Hypertension with CNS signs is a life-threatening emergency.
When to Consider Referral
Naturally, referral is required for cases in which hypertension is suspected and blood pressure cannot be measured. If blood pressure can be measured, the severity of clinical signs will determine whether referral is necessary. Certain concurrent illnesses may also significantly complicate management of the case; such illnesses include advanced renal failure, since too rapid a reduction in systemic blood pressure could lead to acute renal failure. Generally, if signs are mild and include only retinal changes, cases can be handled without referral. For cases in which neurologic signs or severe renal failure is present, aggressive therapy and access to 24-hour care and monitoring are essential.
When Referral Is Not an Option
Which treatments are appropriate when referral is not possible depends on the ability to monitor the patient. If frequent ECG and blood pressure monitoring are not possible, such medications as nitroprusside or hydralazine are best avoided because of their potential to do considerable harm (exact titration is necessary to achieve therapeutic benefit and to avoid significant and potentially dangerous hypotension).
With many cases of hypertension, ACE inhibitors (enalapril 0.5 mg/kg Q 12-24 H in dogs, Q 24 H in cats; benazapril 0.5 mg/kg Q 24 H) can be given, although renal function and electrolyte status need to be carefully monitored, especially if there is preexisting renal disease. Effect on blood pressure is usually quite modest-decreases of 10 to 15 mm Hg are common.
The drug of choice to treat hypertension in cats is amlodipine. The initial dose is 0.625 mg/cat once daily. The dose can be increased to 1.25 mg/cat up to twice daily if needed (a higher dose is commonly needed in patients with a body weight greater than 4.5 kg). Doses in dogs have not been established, although 0.05 to 0.1 mg/kg once or twice daily is a starting point. The dose can be titrated upward if needed, and doses up to 0.25 mg/kg have been recommended.
Monitoring renal function is vital when hypertension is being treated. The frequency with which blood analysis will need to be performed depends on many things, including the presence of preexisting renal disease and how aggressively blood pressure is being lowered. Certainly, when therapy is being initiated, renal blood chemistry parameters should be checked at least weekly.
The Referral Process
If a patient is to be referred, sharing all clinical information is vital, especially blood analysis and imaging study results. If changes are noted on auscultation, documenting the history of cardiac abnormalities and accurate assessment of the case are important.