How to Get the Most from Skin Biopsies
Gail A. Kunkle, DVM, Diplomate ACVD, University of Florida
This article covers what and when to biopsy and how to get the most from your biopsy specimens. A subsequent article will discuss specimen collection with punches or excision.
Find a Pathologist
Foster a working relationship with a pathologist who takes a special interest in dermatopathology-you may need to consult a local American College of Veterinary Dermatology diplomate for a recommendation. A reasonable turn-around time for test results and a written report is 7 to 10 days. Special stains should be done without long delays. The pathologist should provide a morphologic description of the skin specimens submitted and suggest possible causes or pathologic processes.
It is your responsibility to consult resources to determine the next steps based on the pathologist's written report. Like other diagnostic tests, the written results need interpretation. The pathologist provides an expert opinion, but ultimately you must diagnose and treat the patient.
What to Provide Your Pathologist
Give the pathologist properly collected specimens and a detailed description, including data on signalment (age, breed, and sex), age of onset, location of lesions, seasonality, affected family members, and the presence or absence of pruritus. Outline a brief summary of the clinical history with the chronology of the development of lesions and how they relate to clinical signs. If the animal has had prior response to therapy, indicate the medications given. Include your differential diagnoses. Use the submission form provided by your pathologist.
Include a description of each lesion that has been sampled. Ensure that the pathologist can orient each piece of tissue that is taken. Draw pictures on the submission form for clarification. With the availability of digital cameras it is reasonable to send pictures of the lesions and/or the areas sampled. It is important to indicate to the pathologist what you are hoping to rule out.
Sample Collection
For histopathology (and not culture), do not scrub or disinfect the sample site before collection. The type of keratin plus the presence of surface crust, scales, and any organisms or parasites are important and should be preserved. Carefully clip the hair, avoiding trauma to the skin. Hairs should be visible so that the pathologist can orient the specimen correctly.
For collection of most samples, use a disposable 6- or 8-mm biopsy punch along with small, sharp scissors or a blade for cutting the bottom of the specimen away from the patient. Sharp disposable biopsy punches are generally not useful for more than two or three biopsies. Use a scalpel for collection of wedge-shaped samples, which often are needed for nodular or deeper lesions. A scalpel also can be used to make an elliptical incision to harvest vesicles or bulla.
Preserve the integrity of the tissue by placing the sample in the formalin fixative soon after collection. Once placed in formalin, tissue turns a uniform color, and erythema and lesions are not easily seen. Most biopsy sites should be sutured closed. Cauterized tissue should be avoided because it has limited diagnostic use.
Recommendations for Biopsy
Collect samples from diseased skin sooner rather than later. Eliminate secondary infection (bacterial or yeast) first, especially in chronic cases. Cytologic evaluation of the skin can usually help you decide if antibiotics or antifungal treatment is best. In some cases, both are necessary. Repeat the evaluation before collecting specimens in these cases. Remember, for many chronic conditions biopsy may be useful only to rule out certain disorders, such as neoplasia.
It is often helpful to collect several skin specimens that represent various lesions as well as the way you believe the lesions progress in their development. Collect lesions that are representative of the entire process if possible. It is usually only necessary to sample abnormal skin; however, specimens from normal skin may be helpful when evaluating various scaling disorders such as primary seborrhea, depigmenting lesions, various hyperpigmenting lesions, and alopecia. Consult your pathologist.
What to Biopsy: An Illustrated Guide
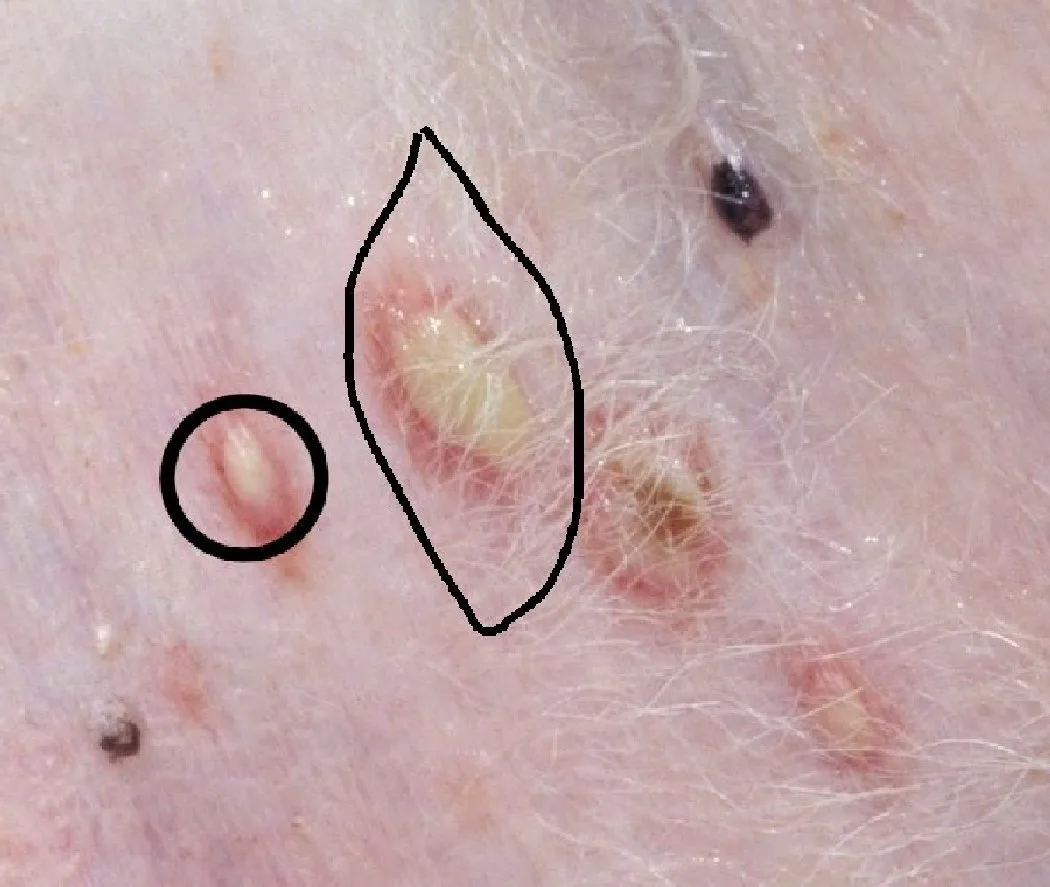
The circles in the figures indicate recommended biopsy sites.
Sample primary lesions whenever possible. Primary lesions include papules, pustules, bullae, nodules, vesicles, macules, plaques, wheals, and tumors. Special care must be taken to preserve the architecture of pustules, papules, vesicles, and bulla. The entire lesion should be removed with a large punch or with wedge excision. Care should be taken not to break the lesion with the rotational movement of the biopsy punch. These pustules would be harvested with a 6- to 8-mm skin biopsy punch or via an elliptical incision.

Collect a specimen from any lump, bump, nodule, or palpably infiltrative lesion. Cytologic studies may be useful, but biopsy is usually required to rule out neoplasia and to evaluate granulomatous lesions and their various causes. Several biopsies for culture may also be needed, depending on the clinical presentation. For deep or infiltrative lesions, take care to collect the deep margin of affected tissue if possible.

Collect a specimen from any cutaneous condition that appears in a geriatric dog or cat without a history of skin disease. This elderly cocker spaniel has generalized scaling and erythema caused by epitheliotropic lymphoma.

Sample ulcerative cutaneous lesions if they are large or there is no history to suggest their cause. When sampling an ulcerated area, try to collect a specimen from the edge of the lesion with some normal tissue or adjacent nonulcerated tissue (include epidermis). In some cases, the best way to do this is with an elliptical incision. The normal tissue is located at the tapering edges, and the ulcer or erosion is in the center.

If you suspect a deep vascular lesion, collect samples from the central portion of an ulcerated lesion. If you suspect vascular disease, take care to confirm that clotting is normal before biopsy. Deep vascular lesions may not be identified with a biopsy punch; a deep wedge biopsy that spans normal and abnormal tissue may be necessary. Several biopsy specimens are often needed for the diagnosis of vasculitis.
Procedure Pearl
Gentleness in collecting and handling the skin biopsy specimen cannot be overemphasized.


Sample any unusual appearing cutaneous condition, especially if there are concurrent physical signs. These footpads are representative of metabolic epidermal necrosis.

Collect a specimen if the primary differentials are conditions that require an owner to commit to expensive or long-term medical management. This is a case of inherited ichthyosis.

Collect a sample from any patient with clinical signs suggestive of a disease best diagnosed by biopsy. Footpad or nasal planum abnormalities, pigmentary alterations, suspect follicular dystrophies, possible genodermatoses, and scaling dermatoses in a breed exhibiting sebaceous adenitis are all examples. This is a case of dermatomyositis in a young collie.

Sample any cutaneous condition that appears to be worsening despite therapy. This may not produce a diagnosis; however, it may help to rule out important differential diagnoses. These lesions, which were originally diagnosed as pyotraumatic dermatitis, worsened with corticosteroid therapy. The definitive diagnosis was calcinosis cutis.

If you are providing normal skin, place the normal specimen in a separate container and label accordingly.

Performing a skin biopsy of the planum nasale that has pigmentary and/or architectural changes is a matter of clinical judgment. Biopsies of the junction as well as those of lesionally representative areas may be beneficial. For the planum nasale and pinna, 4-mm punch biopsies do not yield as large a specimen but may be the preferred option for cosmetic reasons.
