Histiocytic Sarcoma Imaging in Dogs
Casey J. LeBlanc, DVM, PhD, DACVP (Clinical Pathology), Eastern VetPath, Bethesda, Maryland
Christine Mullin, VMD, DACVIM (Oncology), BluePearl Pet Hospital, Malvern, Pennsylvania
Craig A. Clifford, DVM, MS, DACVIM (Oncology), BluePearl Pet Hospital, Malvern, Pennsylvania
Anthony J. Fischetti, DVM, MS, DACVR, Schwarzman Animal Medical Center, New York, New York
Histiocytic sarcoma is an uncommon neoplasm of dendritic cell origin that occurs more often in dogs than in cats,1-5 with Bernese mountain dogs, flat-coated retrievers, Labrador retrievers, and golden retrievers overrepresented.3-5 Presentations may be localized, disseminated, and/or hemophagocytic.1,2 Histiocytic sarcoma can originate from any tissue, although lymph nodes, spleen, subcutaneous tissue, muscle, and periarticular tissue are the most common primary sites.1-5
Cytology or histopathology can often help with definitive diagnosis; immunocytochemistry or immunohistochemistry may be required for differentiation from other round cell tumors and sarcomas.1,2,6,7 CBC, serum chemistry profile, 3-view thoracic radiography, and abdominal ultrasonography should be performed. CT and MRI can also be used if available.3,4 Results can help determine whether disease is localized or disseminated, predict prognosis, and direct recommendations for appropriate therapy. Due to the tumor’s high metastatic rate, treatment for localized histiocytic sarcoma typically involves local tumor control through surgery and/or radiation therapy, followed by systemic therapy with lomustine alone or in combination with doxorubicin or other cytotoxic agents (eg, epirubicin).8-14 The disseminated form is typically treated only with systemic therapy (ie, lomustine alone or in combination with other drugs).3-5,11-14
Hemophagocytic histiocytic sarcoma is a highly aggressive subtype that arises from splenic red pulp or bone marrow macrophages and can only be definitively diagnosed via immunohistochemistry (major histocompatibility complex class II beta integrin, CD11c); however, clinical factors and hematologic and/or serum chemistry abnormalities (eg, hypoalbuminemia, hypocholesterolemia, thrombocytopenia, anemia) may be suggestive of hemophagocytic histiocytic sarcoma, which is associated with a grave prognosis and poor response to therapy.1-4
Histiocytic sarcoma can be challenging to diagnose because of its various forms and clinical presentations. Physical examination, laboratory analysis (eg, CBC, serum chemistry profile, urinalysis), cytology/histopathology, and imaging modalities are key to timely and accurate diagnosis. Continued improvement of therapeutic options is needed to improve prognosis, as most survival times range from only weeks (for hemophagocytic histiocytic sarcoma) to 1 to 1.5 years (for localized histiocytic sarcoma), and curative outcomes are rare.3,5,8-11

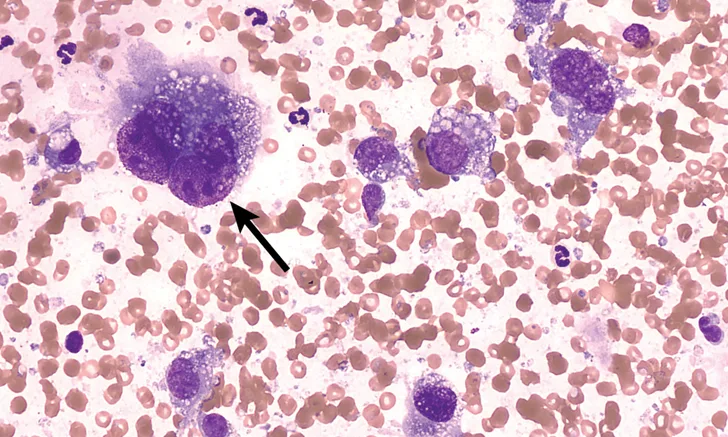
FIGURE 1
Fine-needle aspirate of a cranial mediastinal mass in a 10-year-old spayed schnauzer. Peripheral blood surrounds several irregularly shaped cells with abundant vacuolated cytoplasm and round to irregularly shaped nuclei of variable size (moderate to marked anisokaryosis). These nuclei exhibit finely to coarsely stippled chromatin and occasional prominent nucleoli of variable shapes and sizes. The largest cell is binucleated (arrow), which is a common feature of histiocytic sarcoma.