Head Tilt & Nystagmus
A 10-year-old, castrated male German shepherd presented for acute onset of vestibular disease.
History. The owner observed an acute pain response while petting the dog's head the day before presentation. That night, the owner awoke and found the dog in lateral recumbency, unable to stand or walk. The dog currently was receiving chemotherapy for cutaneous lymphoma and was in clinical remission.
Physical Examination. Findings were as follows: spontaneous rotary nystagmus with fast phase to the right; severe head tilt to the left with a left ear droop; normal reflexes in all limbs; and normal proprioception. The dog was unable to stand without assistance. No other neurologic deficits were noted. Observation of outer left ear pinnae and external meatus revealed a moderate amount of foul-smelling, yellowish-tan purulent discharge. The left vertical and horizontal canals were not visualized with an otoscope due to excessive exudate and discomfort. The right ear was within normal limits.
Laboratory Work. Cytologic ear evaluation; bacterial culture and sensitivity; CBC, chemistry panel, and urinalysis (minimum database for patient of this age to undergo anesthesia); CT; deep ear flush; and repeated otoscopic examination
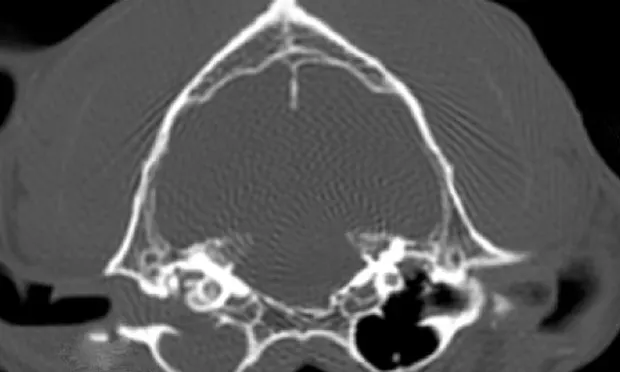
Cytology of the left ear showed too-numerous-to-count bipolar rods and degenerative neutrophils (Figure 1). A CT scan was recommended over radiographs because of its availability, the history of cutaneous lymphoma, and to rule out neoplasia of the ear canal (Figure 2). The CBC revealed a mild leukocytosis with mild neutrophilia and was consistent with a stress leukogram. Chemistry panel and urinalysis were within normal limits. Gentle deep ear flush was done repeatedly with warm saline to clear the exudate. The canal was erythematous, inflamed, and ulcerated, and the tympanic membrane was not visualized. Bacterial culture of the left middle ear exudate produced heavy growth of Pseudomonas aeruginosa. Following the deep ear flush, the left ear was reexamined with the video otoscope (Figure 3).
ASK YOURSELF ...• What neurologic findings help to localize a lesion to the right or left side and to determine if the lesion is peripheral or central in origin?• What are the differential diagnoses?• When is it necessary to culture? What do cytologic studies of the ear reveal?
Diagnosis: Otitis media/interna due to P. aeruginosa with secondary peripheral vestibular disease affecting cranial nerve 8
Interpretation and Treatment. Neurologic examination supported a peripheral origin of vestibular disease. Ear infection was suspected to be affecting the sensory receptors in the vestibular labyrinth and the vestibulocochlear nerve (cranial nerve 8). Although the clinical signs of vestibular disease were acute in onset, the otitis media was probably a chronic problem with no prior clinical signs. CT showed that the exudate extended from the bulla to the external meatus. The deep ear flush revealed no masses in the canal or bulla, and the exudate was removed. It was suspected that the organism was P. aeruginosa because of the bipolar-shaped rods and the nature and odor of the purulent exudate.
Triz-EDTA (DermaPet-Potomac, MD) was instilled under anesthesia and left to stand for 10 minutes. Neomycin, polymyxin B, and hydrocortisone 1% (Cortisporin-Monarch, Bristol, TN) otic preparation and 10 drops of fluocinolone acetonide and dimethyl sulfoxide (Synotic-Overland Park, KS) were instilled into the middle ear.
The patient made an uneventful anesthetic recovery and remained in the ICU for 3 days due to severe vestibular disease, during which time treatment consisted of enrofloxacin 20 mg/kg IV daily and Triz-EDTA, neomycin, polymyxin B, and hydrocortisone 1% twice daily. On day 3, the dog was able to stand and walk with support. It was discharged with oral ciprofloxacin 20 mg/kg/day PO for 9 weeks. Topical therapy was continued twice daily until week 4, when the tympanic membrane was visualized and cytologic studies were negative. The underlying reason for the unilateral ear infection was not determined; however, immune suppression from chemotherapy was suspected.
DID YOU ANSWER...• Peripheral disease. Generally head tilt is toward the side of the lesion without other neurologic deficits (e.g., hypometria, hypermetria, or proprioceptive deficits). In addition, nystagmus is horizontal or rotary in nature. Other neurologic signs with secondary otitis media/interna are Horner's syndrome and facial nerve paralysis. Horner syndrome occurs because the sympathetic fibers to the eye pass though the middle ear, whereas the facial nerve passes through the inner ear.
• Central disease. If the vestibular nerve at the level of the medulla (central) is involved, the head tilt may still be toward the lesion but with additional neurologic defects (i.e., proprioceptive deficits). In paradoxic cerebellar central disease, head tilt can be toward the opposite side of the lesion and occur with other central neurologic defects (i.e., hypermetria). A dog with central vestibular disease exhibits additional neurologic signs, such as proprioceptive deficits, hemiparesis, or quadraparesis, which may support a brainstem lesion. Nystagmus in central disease is most often vertical, positional, or rotary. Head tremors, hypermetria, or hypometria would provide evidence of a cerebellar lesion. Altered mentation may also be evident in central disease.
• Otitis media/interna, idiopathic vestibular disease, neoplasia (middle/inner ear), foreign body.
• Culturing is necessary when rod-shaped bacteria are seen on cytologic studies to rule out Pseudomonas species. Cytology can provide important information on the type of infection. Cocci-shaped bacteria are most likely indicative of Staphylococcus intermedius; peanut-shaped yeast organisms are Malassezia species.