Femoral Head & Neck Ostectomy
Laura E. Peycke, DVM, MS, DACVS, Texas A&M University
Femoral head and neck ostectomy (FHO) is a commonly performed procedure for surgical treatment of traumatic and chronic conditions affecting the hip.
The option to do an FHO is typically presented along with other surgical alternatives. Some surgeons see it as a last resort or a “salvage” procedure, whereas others believe it to be a primary recommendation for many orthopedic diseases of the hip.
Indications
Common indications for an FHO include:
Femoral head and neck fractures
Catastrophic acetabular fractures
Coxofemoral hip luxations
Failed total hip replacements
Chronic pain associated with hip degenerative joint disease (including traumatically induced disease, Legg-Perthes disease, and canine hip dysplasia)
Excision of the femoral head and neck palliates pain by eliminating bony contact between the pelvis and femur, allowing formation of a pseudoarthosis. The pseudoarthrosis that forms comprises dense fibrous tissue lined by a synovial membrane.
Author Insight
A thorough review and understanding of the craniolateral approach to the hip is recommended. Preservation and reconstruction of the supportive soft tissues are keys to a quick return to ambulation and long-term function. Recognition of the origin and insertions of the hip musculature is especially important if the FHO is performed on a hip that is luxated or traumatized.
Outcome
The procedure has the best outcome and is typically recommended for mature pets and dogs weighing < 17 kg; however, physically fit dogs of all sizes tend to rehabilitate and respond favorably regardless of their weight. In addition, muscle mass has been found to be one of the most important variables in determining outcomes of the procedure.
Postsurgical FHO patients have some degree of limb shortening and gait abnormality; however, with aggressive rehabilitation, these animals have been reported to respond well to the procedure and return to an active lifestyle.
Step-by-Step: Femoral Head & Neck Ostectomy
Step 1
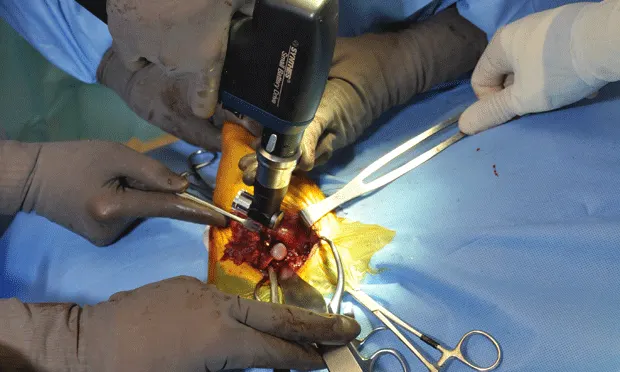
The animal should be routinely anesthetized using a premedication, an induction agent, and gas anesthesia; then placed in lateral recumbency with the affected limb hung and aseptically prepared for surgery (A).
The hip is then draped routinely to allow manipulation of the limb. A proper craniolateral approach to the hip is dependent on the identification of the ischial tuberosity (white arrow), the greater trochanter (arrowhead), and iliac wing of the pelvis (red arrow) (B).


Step 2
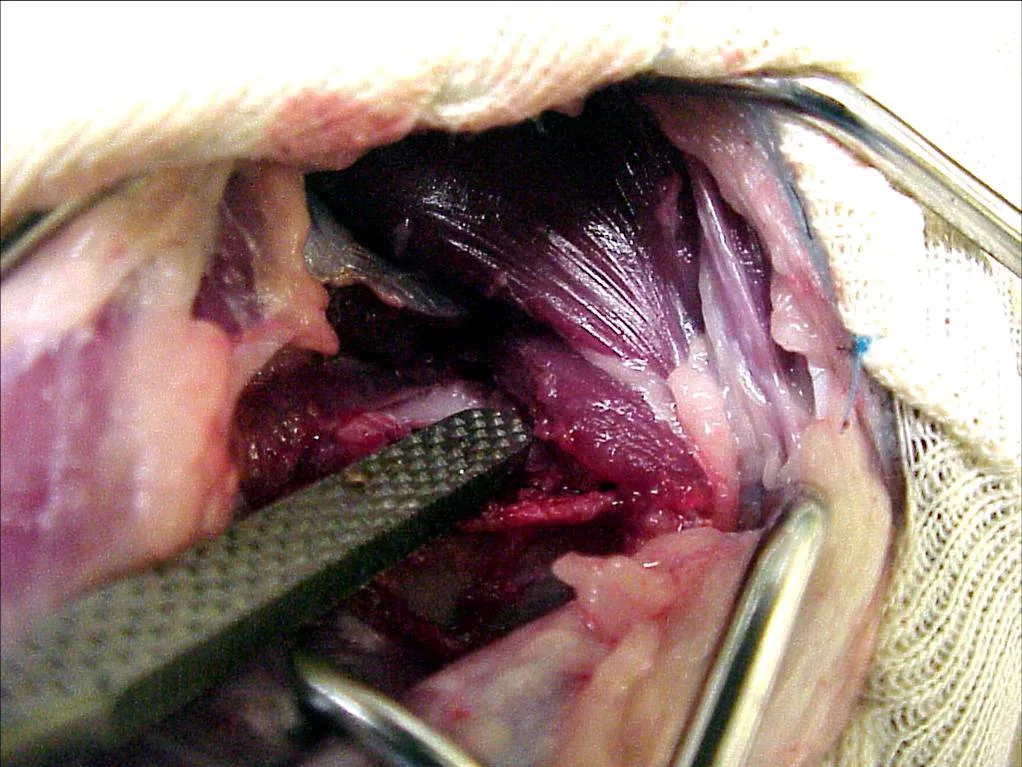
The skin incision should be made slightly cranial to the greater trochanter in a proximal to distal direction. The biceps femoris, tensor fascia lata, and gluteal musculature should be identified and minimally disrupted until the muscular planes are appreciated. The plane between the tensor fascia lata and biceps femoris are incised and separated. The tensor fascia can then be retracted cranially, whereas the biceps musculature is retracted caudally. The superficial and middle gluteal muscles (arrow) are identified and retracted dorsally without excision of the musculature or tendinous insertions. The deep gluteal muscle is identified by the arrowhead.

Step 3
At this point, identification of the tendon of the deep gluteal muscle (arrow) is possible (A). Gentle elevation (with a periosteal elevator) of this tendon allows partial tenotomy and identification of underlying hip joint capsule. The joint capsule can then be identified and incised in a radial fashion along the acetabulum and onto the femoral neck. Continuation of the incision along the origin of the vastus lateralis is recommended. Elevation of the vastus lateralis musculature can be performed and should be extended until full exposure of the femoral neck is accomplished (B).
Author Insight
Because the hip has been draped “out,” movement of the hip and easier identification of the hip joint are possible. Effective use of assistants and additional Gelpi and Hohmann retractors are important for visualization and adequate exposure of the femoral head and neck. When using pointed retractors, care must be taken to avoid trauma to the sciatic nerve, which is located caudally in relation to the hip joint.


Step 4
The head of the femur is freed from the remaining joint capsule and round ligament with curved Mayo scissors or a Hatt spoon. Complete excision of the round ligament is important to allow disarticulation of the hip and protection of deep structures when excising the femoral head and neck.
Step 5
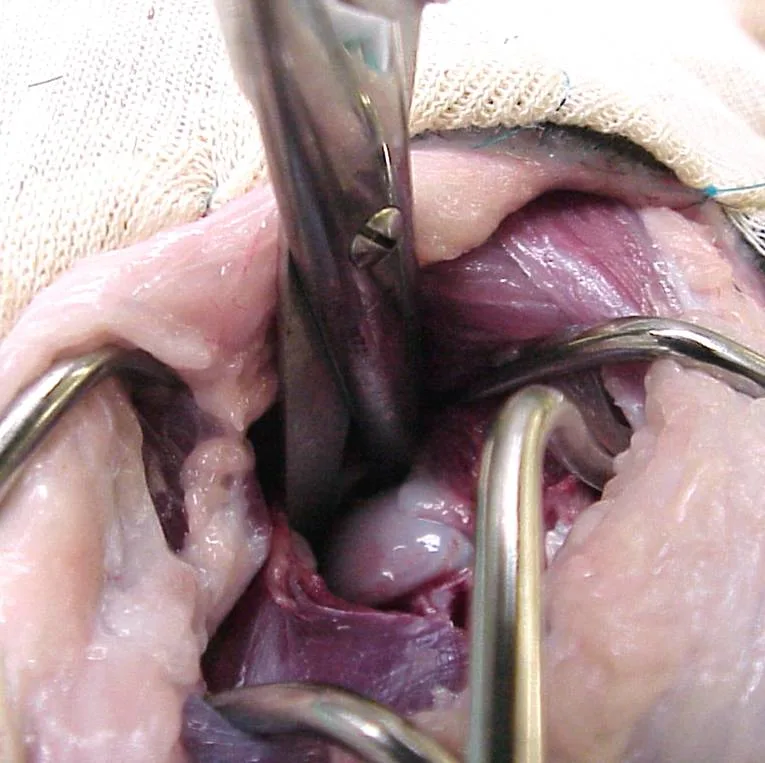
Landmarks for the femoral head and neck are now visible and include the medial aspect of the base of the greater trochanter (arrow) and lesser trochanter (arrowhead), located on the medial cortex of the femur. With adequate elevation of the origin of the vastus lateralis muscle, direct palpation of the lesser trochanter is possible and should be performed. The lesser trochanter is best appreciated as a small “bump.”
The insertion of the iliopsoas muscle is also palpable at or slightly distal to the lesser trochanter. Ideally, this muscular insertion is preserved during the excision of the femoral neck, but not at the expense of eliminating bony contact of the medial femoral cortex with the pelvis.
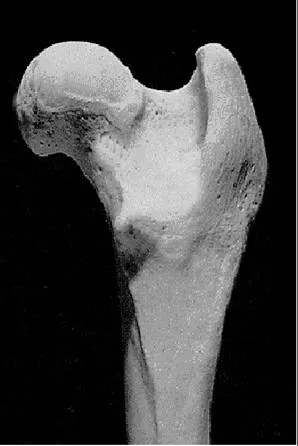
A shows the femoral head and neck prior to ostectomy; B shows how the femur should look when the correct cut is made during ostectomy.
Author Insight
To position the saw or osteotome and perform adequate excision of the femoral neck, the limb must be maintained in external rotation so that the knee is positioned at 90 degrees to the table while the cut is being made. An assistant can help the surgeon maintain the limb in the proper position.

Step 6
Once the parameter for the femoral neck is appreciated, a line may be marked for accurate positioning of an osteotome (at least 2- to 3-cm wide) or power saw. The cutting device should be positioned on this line and then tilted toward the patient’s head so that the ostectomy is being directed in a caudal and medial direction. This ensures adequate bony tissue will be removed on the most caudal and medial aspect of the femur.
The tendency to position the osteotome or saw in a perpendicular position in relation to the femoral neck will lead to incomplete excision of the femoral neck and could result in residual contact between the femur and pelvis. The orientation of the cutting instrument should be tilted a few degrees toward the dog's head.
Step 7
Prior to the ostectomy, Hohmann retractors can be placed on both the cranial and caudal aspects of the femoral neck. These retractors will help with tissue retraction and protect the sciatic nerve and underlying soft tissues. With external rotation of the limb being maintained, the cut is made.

Step 8
Once the cut is completed, the tissue to be removed is grasped with a bone-holding forcep. The femur is then carefully palpated for residual bony prominences or irregularities. The hip is placed through a thorough range of motion. Any “grinding” or bony contact between the femur and hip should not be ignored.
At this point, the use of rongeurs or a rasp can be used to excise remaining tissue and to smooth rough surfaces (A). Inspection of the resected femoral head and neck can give some insight as to whether additional tissue needs to be excised (B).

Author Insight
When palpating the hip joint, free movement should exist through a complete range of motion. Careful debridement with rongeurs on the medial cortex can assist with elimination of bony contact.

Step 9
Once smooth range of motion has been acquired, closure of the hip may be performed. Interpositioning of soft tissue between the femur and acetabulum may be performed at this stage but remains controversial; proponents believe this additional step increases the soft tissue “padding” between the ostectomy site and pelvis. A positive outcome has been noted in short-term reports; however, there is no reported difference in long-term outcome.
In my experience, this technique not only requires additional soft tissue dissection and is unnecessary for long-term positive results but may also increase the chances of deep tissue necrosis and infection.
Author Insight
Orthogonal view post-operative radiographs should always be taken to ensure adequate excision of the femoral head and neck.

Step 10
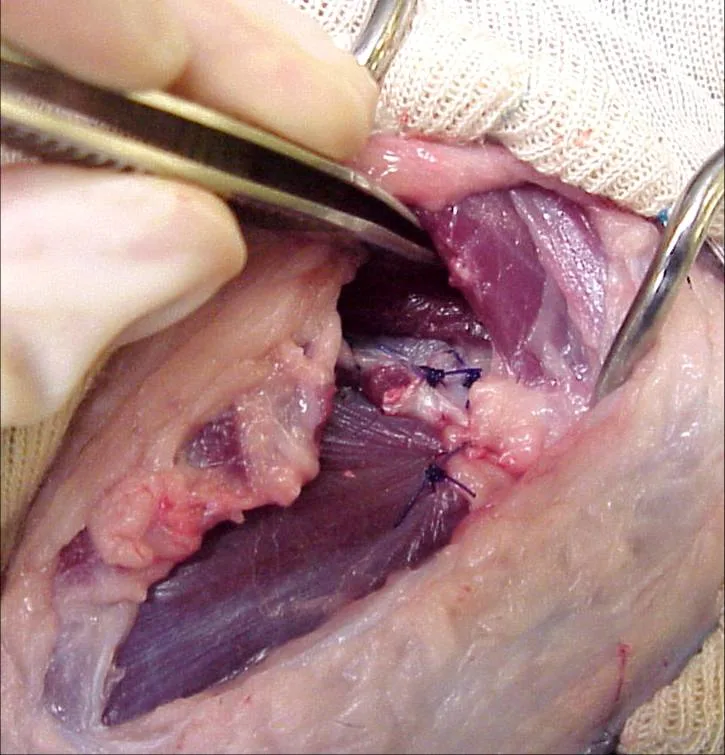
Prior to closure, the surgical area should be flushed with sterile saline. Closure can be performed by closing any residual joint capsule over the acetabulum using 0 or 2-0 absorbable suture. One or 2 mattress sutures can then be placed in the deep gluteal tendon to repair the previous tenotomy site. The vastus lateralis can then be reattached to the deep tissues by using simple interrupted sutures. All other superficial tissues are closed routinely.
Postoperative Care
The postoperative period is extremely important to the recovery and return to function. It is critical to the success of the procedure to be clear about the rehabilitation plan with the client.
Rehabilitation in the form of passive range of motion and controlled activity is encouraged and should be explored within the first days after surgery.
Swimming is also acceptable during rehabilitation but should be postponed until after the incision has healed.
Ice and heat therapies, along with antiinflammatory medications, can be used to assist with pain management.
Frequent rechecks to ensure maintenance of hip range of motion should be performed.
Complications
Complications associated with FHOs include decreased range of motion (especially abduction and extension of the hip), limb shortening, muscle atrophy, infection, and loss of function. A recent study reported that there may be discrepancies between the results of objective clinical data and subjective observations by owners, but a high degree of owner satisfaction was reported following FHO.
Prognosis
If an FHO is performed properly (adequate ostectomy and careful soft tissue manipulation) and followed by aggressive rehabilitation, a positive outcome can be expected; however, bony regrowth is sometimes seen in dogs younger than 9 months of age.