FIP is a global disease that traditionally affects kittens; however, with the proper combination of exposure, genetic predisposition, and random mutational events, cats of any age can be affected. The mortality rate has been defined as ≥95%, but recent advancements in antiviral drug therapy have created the potential for effective treatment.1,2
Background & Pathophysiology
FIP is caused by infection with a mutant biotype of feline enteric coronavirus (FECV), which can lead to various complex clinical signs.3-5 FECV infection rates vary significantly across populations. Infection occurs in ≈40% of cats worldwide and 90% to 100% of cats in multicat households3,6; however, only a small percentage (<10%) of cats develop FIP.
The pathogenesis may be difficult to explain to pet owners. In addition to virus exposure, FIP development depends on environmental stressors, genetic predisposition, and random viral mutation. The disease is complex and can be best understood when described as a series of steps3,4,7:
Cats are exposed to FECV, which enters enterocytes using a spike (S) protein gene on the viral surface. Usually, FECV causes self-limiting gastroenteritis that is often undiagnosed. FECV may also spread systemically without causing FIP.5
In some cats, the S protein gene mutates—the viral 3c gene may also be truncated—causing tropism to change from enterocytes to macrophages/monocytes; this mutated virus is referred to as FIP virus (FIPV). The mutated virus replicates within immune cells and is no longer transmissible through the fecal–oral route.
In some cats, a strong cell-mediated immune response can control infection, resulting in viral clearance without clinical disease. If a humoral response predominates, antibodies are ineffective at controlling infection and can lead to immune complex formation, resulting in vasculitis and effusion (ie, wet FIP). In the case of a partial cell-mediated immune response, immune cells are recruited to the site of replication, leading to granuloma formation (ie, dry FIP). The distinction of wet versus dry FIP depends on the ratio of cell-mediated (Th1) and humoral (Th2) responses.8
Both wet and dry forms of FIP result in death if left untreated.
A genetic predisposition to FIP,9,10 wherein decreased gene heterozygosity may contribute to an altered immune response to FIPV, is likely to occur.2 This may explain the apparent predisposition of purebred cats to development of disease.9
History & Clinical Signs
FIP typically affects cats <3 years of age, with a second smaller peak in prevalence in geriatric cats6; however, cats of any age can be affected.
Dry FIP can manifest with organ dysfunction, uveitis, neurologic signs, fever, anemia, and/or lethargy and is caused by granulomas or immune complex deposition. Cats with wet FIP may have ascites or pleural effusion in addition to the aforementioned signs (Figure 1). Clinical presentation can vary from minor to life-threatening and involve almost any organ system.
Many cats with FIP are febrile, but fever can wax and wane. Globulins are classically elevated, often significantly (ie, >7 mg/dL), and albumin is typically normal to low (ie, 2 mg/dL or less). Mild to moderate anemia (ie, hematocrit, 20%-30%), RBC microcytosis, band neutrophilia, and lymphopenia are common; hyperbilirubinemia (as a result of hemolysis) and hyperglobulinemia are also often observed. The albumin:globulin ratio is classically <0.4.5,11,12 Lymphopenia and hyperbilirubinemia are more prevalent in wet FIP.
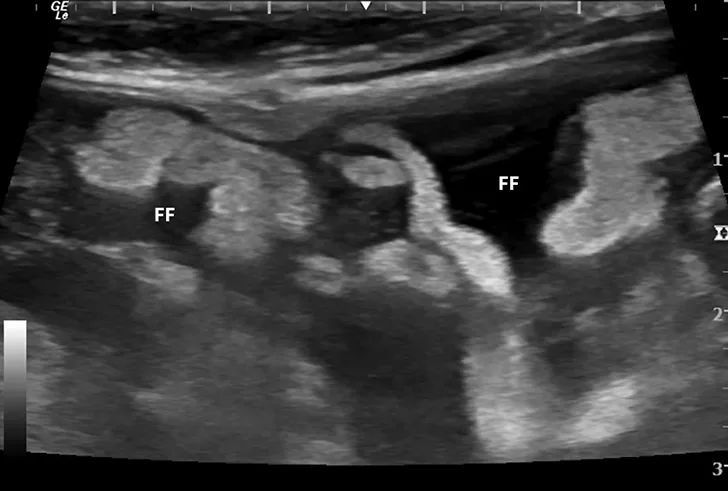

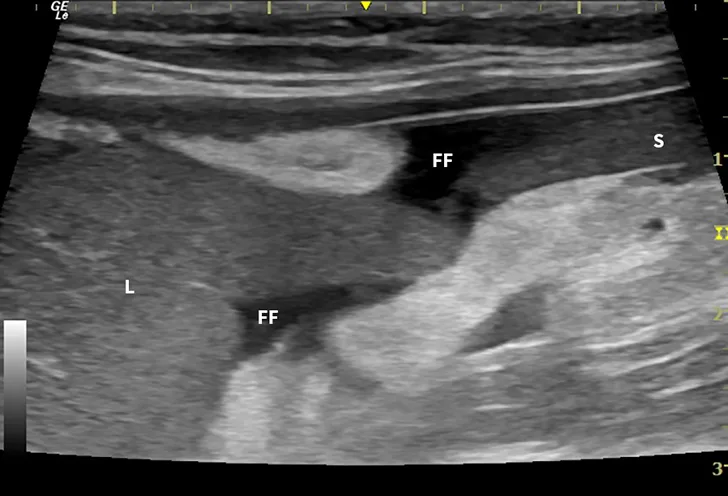

Ultrasound image showing abdominal effusion in a cat with wet FIP. Anechoic fluid is present between organs, distending the abdomen. FF = free fluid; L = liver; S = spleen; K = kidney
Diagnosis
Serology for FECV is rarely beneficial,6 as serology cannot distinguish FECV and FIPV antibodies, and some cats with FIP may test negative on ELISA,5,13 which has poor sensitivity for immune complexes. Serology is likely only useful on a population level as a screening tool for coronavirus exposure. No evidence indicates that the viral 7b protein ELISA is superior to other antibody assays.14
Immunohistochemical detection of coronavirus within lesions is the gold standard for diagnosis of FIP,5,15 but collection of tissue samples is often impractical because of the need for anesthesia and surgery. Diagnosis is also possible using cytology from ultrasound-guided aspiration of enlarged mesenteric lymph nodes.5,16
Wet FIP is often readily diagnosed through sampling of effusion, which is typically straw-colored, translucent, and slightly more viscous than water. Fluid generally has low cellularity that consists of mildly degenerate neutrophils and macrophages.
Dry FIP often requires more advanced diagnostics, including tissue aspiration or biopsy. A wide range of diagnostics have been suggested, including routine serum chemistry profiles, diagnostic imaging, measurement of acute-phase proteins, PCR, and cytology. In the absence of immunohistochemistry, combinations of methods are often used to diagnose patients with a high degree of certainty. Consistent nonspecific clinical pathologic findings (Table) should raise suspicion for FIP.6
Table: Clinical Pathological Findings in Cats With FIP*,12
*Not all changes are seen in every cat, and some cats may show no changes. Changes also depend on presentation (wet vs dry).
The Rivalta test (Figure 2) is an inexpensive and readily performed in-clinic test with an extremely high negative predictive value for FIP.5,13 This test is positive in effusions with high protein content (especially acute-phase proteins) and negative in pure transudates. A positive Rivalta test is consistent with FIP in kittens but is less specific in older cats, as septic peritonitis and neoplasia can result in a positive test; however, these conditions can be ruled out via cytology.
PCR is a valuable modern tool for FIP diagnosis because it allows direct detection of viral RNA; some experts question its use in all cases, but most consider it to be a useful tool. Detection of FECV by PCR in tissue or effusion is consistent with FIP but not definitive, as non-FIP FECV may also be present in the tissue of healthy animals; however, failure to detect FECV can indicate that FIP is unlikely.7 Some specific S protein gene mutations are associated with FIP, and PCR tests that target these mutations may have higher specificity17,18 (ie, diagnosis is more likely if the detected virus has one of these mutations). Although potentially clinically useful, PCR testing is not comprehensive because novel mutations may be missed.17,19 PCR testing of feces is not useful because fecal coronavirus is not predictive of systemic spread.
PCR sample choice depends on disease presentation; in cases of wet FIP, effusion should be tested, and in cases of dry FIP, peripheral blood, CSF, aqueous humor, lymph nodes, and/or organ aspirates should be tested.16,20 Test results should be interpreted based on the sample submitted; a positive PCR that identifies specific S protein gene mutations in abdominal effusion likely indicates FIP, but a positive FECV result in peripheral blood is less specific.19,20 It should be noted that testing is done sequentially. Initially, reverse transcriptase PCR for FECV is performed. When the result is positive, a second PCR should be run to confirm the FECV is FIPV, not FECV, biotype.
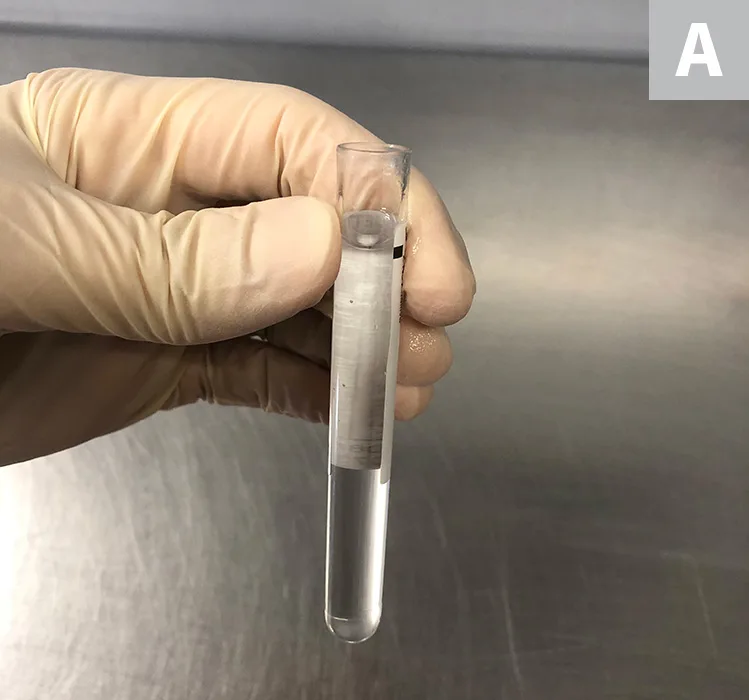
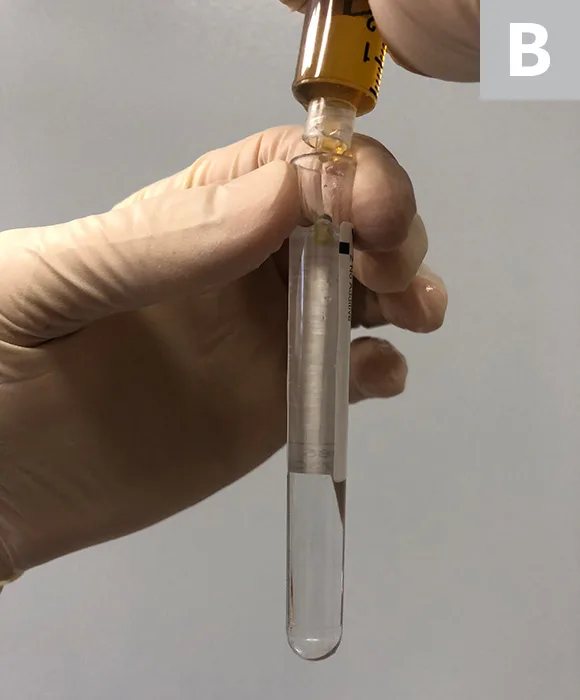
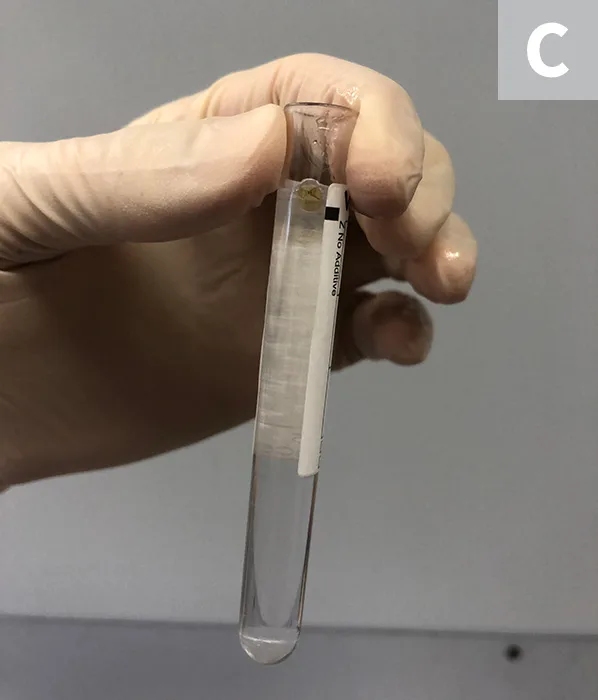
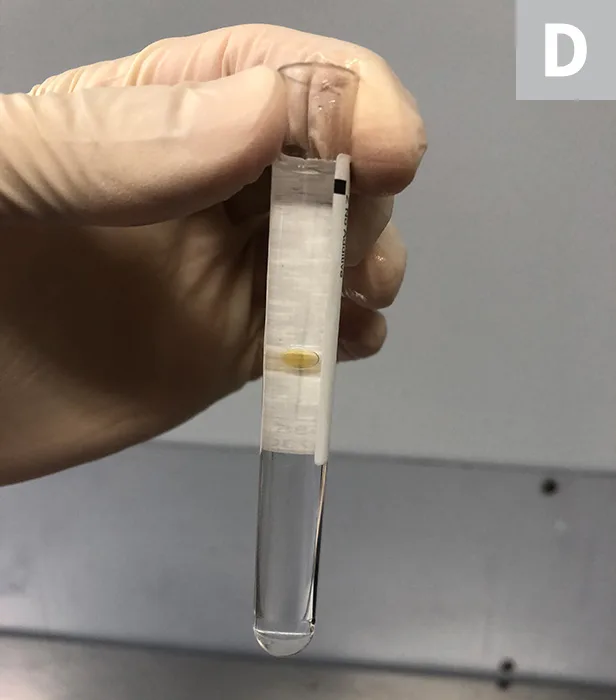
Rivalta test procedure; a quick and inexpensive assay of the inflammatory protein content of a fluid sample. A test tube is filled with 7 to 8 mL of distilled water, followed by the addition of one drop of glacial (anhydrous) acetic acid (A). A drop of effusion is placed on top of the solution (B) and observed; the drop near the top of the tube (C); the drop partway down the tube (D). If the drop retains its shape and slowly drifts to the bottom of the tube or remains suspended, the test is positive. In a negative test, the drop dissolves and the tube appears clear.
Treatment & Management
Treatment of FIP has traditionally been unrewarding, and management of clinical signs and supportive care to keep infected cats comfortable have been the mainstays of therapy. Many clinicians administer corticosteroids to reduce the inflammatory response and improve quality of life, but there is no evidence that this extends survival.21
The use of immunomodulatory therapy—including immunostimulants, type 1 interferons (IFNs; eg, human IFNα, feline IFNω), and other similar drugs22,23 intended to bias toward a Th1 response—has been proposed.21,24 Preliminary data on these approaches have been inconsistent, with some data showing positive effects and others showing no effects.22
Coronaviral protease inhibitors and nucleoside analogs (eg, GC376 and GS-441524, respectively) represent major breakthroughs in therapy.25 These agents inhibit viral replication and disrupt FIP progression, prolonging patient survival.26 The efficacy and safety of these drugs has been confined to laboratory, clinical, and field studies, but commercialization of GC376 is underway. Although not 100% effective, especially with ocular or CNS involvement, these agents are the most promising therapies to date.23,25,27 Unfortunately, none are currently commercially available, but the purchase of research-grade drugs online has been widely reported. The legality, ethics, and efficacy of buying and selling these drugs are beyond the scope of this discussion.
August 2024: Is GS-441524 now an option? Your FAQs answered here.
Prognosis & Prevention
Prognosis for FIP is traditionally very poor (ie, <5% 1-year survival rate).6 Cats with wet FIP are reported to survive only for weeks11; cats with dry FIP have a longer survival time, but this form is also fatal. Newer antiviral therapies may significantly improve prognosis, and longer-term survival is possible.27
Although a vaccine for FIP is available in some regions, its efficacy is poor and it is not generally recommended. Development of an effective vaccine has been unsuccessful due to the genetic variability of the virus and a lack of sterilizing immunity (ie, vaccination does not prevent infection) and antibody-dependent enhancement (ie, pre-existing antibodies may worsen disease through immune complex formation).28
FIP is not directly contagious. FECV is directly contagious and is an enveloped virus with poor environmental survivability; thorough cleaning is needed to disinfect the environment.11 Prevention of coronavirus infection is difficult and can be futile in large groups due to the ubiquity of the virus and number of clinical carriers.
Although diagnosis and treatment of FIP may seem daunting, recent breakthroughs in treatment and understanding have shed light on this previously enigmatic disease. Simple (eg, Rivalta) and more complex (eg, PCR) tests have improved diagnostics, and antiviral drugs show potential for successful therapy.