Chin Dermatitis in a Cat
A 6-year-old, 4.5-kg, spayed Abyssinian cat presented with a 4-month history of progressive chin dermatitis.
HistoryThe owner initially noticed black debris throughout the fur over the chin. During the next 4 months, hair loss developed as a result of the cat scratching the area. Initial prescribed treatment included application of a warm washcloth q12h and topical administration of benzoyl peroxide (2.5%), which appeared to cause clinical signs to worsen.
The cat was indoor only, up-to-date on vaccinations, and the only household pet.
Related Article: Skin Disease in Cats: It Isn’t Always What It Seems
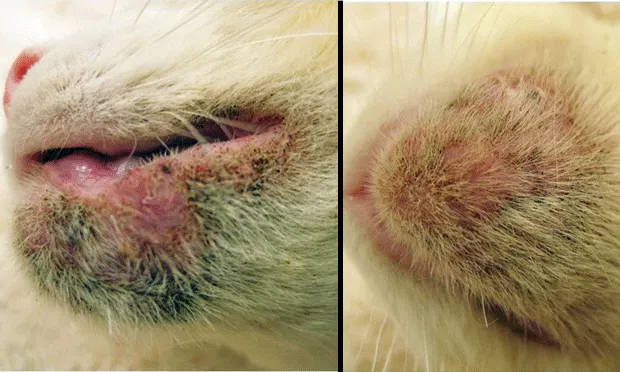
ExaminationOn presentation, the cat was bright, alert, and responsive. There was some scarring over the right cornea from a previously healed ulcer. Comedones, dark keratinous debris, barbered hair, papules, erosions, and swelling were noted over the chin and lower lip; comedones and dark keratinous debris were also noted on the upper lip (Figure 1. Appearance of patient’s chin (A) and upper and lower lips (B) on presentation).
DiagnosticsSkin scrapings were negative for demodectic mites. Cytologic examination of a papular lesion sample revealed coccoid bacteria with suppurative inflammation. Wood’s lamp examination and dermatophyte test medium sample were negative.
The patient was sedated with IM ketamine at 5 mg, dexmedetomidine at 0.03 mg, and butorphanol at 0.5 mg, along with local sedation of lidocaine; two 6-mm punch biopsy specimens with skin were obtained from the chin. Dermatohistopathologic examination revealed comedone formation, mild lymphoplasmacytic periductal inflammation with suppurative folliculitis, and intrafollicular coccoid bacteria.
Ask Yourself:1. What are the differentials for chin dermatitis in this patient?2. What clinical signs are associated with this patient’s condition?3. Where is the ideal site to obtain a punch biopsy specimen for diagnosis?4. What dermatohistopathologic changes would be associated with this patient’s condition?
Diagnosis: Feline acne with secondary bacterial pyoderma
Related Article: Hair Loss in Cats
The cutaneous lesions were consistent with feline acne and secondary bacterial pyoderma and confirmed histologically (see Did You Answer?).
Inmany cases, feline acne is a straightforward diagnosis based on classic clinical lesions (see Clinical Presentations of Feline Acne). However, it is important to rule out demodicosis, ectoparasites, and dermatophytes as underlying causes.


TreatmentA topical agent that inhibits comedogenesis and flushes hair follicles, such as salicylic acid, topical retinoids, benzoyl peroxide, or sulfur, is essential when treating feline acne.
Because many cases of feline acne also include secondary bacterial infection that likely involves gram-positive organisms, topical antimicrobials should be considered, particularly when papules, furuncles, and draining tracts are present. Appropriate topical agents include 2% mupirocin, fusidic acid, clindamycin, tetracycline, erythromycin, and metronidazole. Mupirocin and fusidic acid are ideal choices, as both target gram-positive bacteria. Mupirocin also penetrates deep within the skin, reaching regions of furunculosis.
Ideal first-line systemic antimicrobial agents that can be prescribed for 3 weeks (superficial bacterial infections) to 6 weeks (deep bacterial furunculosis and draining tracts) include cefpodoxime, amoxicillin–clavulanic acid, clindamycin, cefadroxil, cefovecin, and cephalexin.
Bacterial PyodermaMalassezia spp overgrowth or small amounts of yeast can be treated topically with miconazole, clotrimazole, ketoconazole, or chlorhexidine. Severe Malassezia chin dermatitis can be treated with oral itraconazole or fluconazole for 3 weeks. Supplemental fatty acids may reduce inflammation and normalize keratinization long-term. Administration of an omega-3 fatty acid, such as eicosapentaenoic acid (EPA) at 270 mg or docosahexaenoic acid (DHA) at 180 mg q48h, is considered sufficient.
A course of oral prednisolone at 2 mg/kg tapered over 10 to 14 days may be required for cats with marked edema, furunculosis, or scarring. Administration of oral synthetic retinoids (ie, isotretinoin, acitretin) should be reserved for cats that do not tolerate topical treatment or that develop marked refractory acne. Synthetic retinoids are beneficial in treating feline acne, as they demonstrate antikeratinization and antiinflammatory activity and may indirectly reduce bacterial populations in sebaceous pores. Adverse effects reported in cats include blepharospasm, periocular crusting, erythema, anorexia, diarrhea, and weight loss.1 Laboratory parameters that may rarely change include elevated triglyceride and cholesterol concentrations, increased platelet counts, and elevated ALT and AST levels. In addition, it is important to note that synthetic retinoids are known teratogens.
OutcomeThe patient’s chin and perioral regions were clipped to improve efficacy of topical therapy. Alcohol-free pads treated with salicylic acid and aloe vera were administered q24h for 3 weeks. Salicylic acid, an effective follicular flushing agent, is well tolerated by cats. Benzoyl peroxide has been shown to cause irritation in some cats.
Mupirocin 2% topical ointment, which mainly shows activity against gram-positive bacteria, was applied q12h for 3 weeks. Treatment with cefpodoxime at 5 mg/kg q24h for 4 weeks was initiated because some papules had eroded and were draining serosanguineous exudate.
In one study, the most commonly isolated bacteria from cultures were coagulase-positive Staphylococcus spp and a-hemolytic Streptococcus spp.2 Organisms that were cultured less frequently included Micrococcus spp, Bacillus spp, and Escherichia coli.
At 3 weeks, the cat was not pruritic. The comedones, papules, and dark keratinous debris had mostly resolved. The owner was advised to complete cefpodoxime therapy, discontinue mupirocin, and continue cleaning the region with salicylic acid–aloe vera pads 2 to 3 times weekly for maintenance.
Did You Answer?
1. Differentials include feline acne, demodicosis, dermatophytosis, allergic skin disease (atopic dermatitis, food hypersensitivity), eosinophilic granuloma complex (swollen chin), viral infection (feline calicivirus, feline herpesvirus), neoplasia, primary irritant contact dermatitis, and secondary bacterial and Malassezia dermatitis.
2. Feline acne is a disorder of follicular keratinization.3 Many cases progress to and remain in the comedonal stage. In this asymptomatic stage, comedones appear over the chin and occasionally involve the upper and lower lips. Some cases can involve erythema, papules, pustules, alopecia, and pruritus. More severe and chronic cases can involve progression to painful furunculosis with diffuse edema, thickening, fistulation, and scarring.
3. Discrete comedones represent ideal locations for obtaining punch biopsy specimens. Erosions, ulcers, and draining tracts should be avoided.

4. Early dermatohistopathologic lesions involve lymphoplasmacytic periductal inflammation, sebaceous gland duct dilation, and follicular keratosis with plugging and dilation (Figure 3). More advanced lesions show evidence of folliculitis (Figure 4), furunculosis, pyogranulomatous sebaceous adenitis, and dermatitis. Staphylococcus spp organisms and Malassezia spp may be present in comedones and surface crusts.
Figure 3. Histopathology of a comedone specimen (

magnification, 100×)
Figure 4. Histopathology of a comedone specimen showing suppurative inflammation and intrafollicular coccoid bacteria (magnification, 400×)
EDWARD JAZIC, DVM, DACVD, practices at Dermatology for Animals in northern California and Ohio. He has published an extensive review of the clinical, infectious, and histopathologic features of feline acne in Veterinary Dermatology and authored multiple sections and chapters about this topic and others in several veterinary textbooks. Dr. Jazic earned his DVM from University of Illinois.
CHIN DERMATITIS IN A CAT • Edward Jazic
References
1. Acne. Jazic E. In August JR (ed): Consultations in Feline Internal Medicine, vol 6—St. Louis: Saunders Elsevier, 2010, pp 375-381.2. An evaluation of the clinical, cytological, infectious and histopathological features of feline acne. Jazic E, Coyner KS, Loeffler DG, Lewis TP. Vet Dermatol 17:134-140, 2006.3. Keratinization defects. Muller & Kirk’s Small Animal Dermatology, 6th ed. Scott DW, Miller WH, Griffin CE— Philadelphia: Saunders Elsevier, 2001, p 1042.