Cesarean Section in the Dog
Karine J. Onclin, DVM, PhD, DECAR, University of Florida
John P. Verstegen III, DVM, MSc, PhD, DECAR, University of Florida
While cesarean section is a common surgical procedure, it may be associated with significant mortality in both dams and puppies. Timing is extremely critical for puppy survival for both emergency and elective c-sections. If delivery is delayed by more than 24 hours after the start of the second stage of labor, the loss of all puppies due to placental detachments usually ensues. Emergency c-section should be performed as soon as possible after it is determined that labor is unproductive, before the occurrence of dam exhaustion or distress of the puppies and/or the dam.
Close coordination of the surgeon, anesthetist, and nursing staff is critical. Good preparation of the dam, correct selection of the anesthesia protocol, fast surgical delivery, and adequate neonatal care are the keys to complete success. Ideally, the dam should be totally awake as soon as possible after the procedure to allow for development of the neonatal/maternal bond and maternal adoption of the neonates. This point is critical when considering anesthesia and surgical protocols.
Procedure Pearl
It is important to master each of the surgical steps to reduce the length of the procedure.
Preparation of the Dam
Shaving the dam prior to induction of anesthesia reduces the time fetuses are exposed to anesthetic agents.
Maternal oxygenation for 10 to 15 minutes before anesthesia induction (with either a mask or a nasal tube) reduces hypoxia during both intubation and induction/maintenance of anesthesia. It also improves surfactant production in neonates.
Many dams in distress are dehydrated. Establishing an IV line for fluid will help maintain blood pressure and prevent the effects of blood loss.
It is the author's experience that, particularly for elective c-sections, an IV injection of a short-acting corticosteroid such as methylprednisolone (Solu-Delta-Cortef; www.pfizerah.com) 2 to 8 hours before surgery stimulates progesterone decrease, prevents shock development, and stimulates surfactant production in neonates, making the success rate significantly higher. The use of methylprednisolone is essential, particularly if the timing of the c-section is approximate. Since timing can be incorrect due to peculiarities of the dog's cycle, particularly if progesterone plasma concentration has not been monitored to evaluate timing, methylprednisolone may be advisable in most cases.
Selection of Anesthesia
The main concerns when choosing the anesthesia protocol are:
Welfare of dam
Viability of fetuses
Ideally, the anesthetic drugs should:
Not cross the placental barrier (eg, glycopyrrolate vs atropine)
Be short-acting and rapidly or minimally metabolized
Not depend on liver metabolism or renal excretion, both of which are highly deficient in the canine neonate (eg, propofol vs barbiturates)
Be reversible by antagonism (if they are not short-acting) and the antagonist should not have any side effects of its own (eg, benzodiazepines vs phenothiazines)
Provide adequate analgesia for the dam, without affecting the maternal adoption process, maternal behavior, and lactation (eg, opioid injection after delivery of puppies vs the same at induction of anesthesia, a local block vs systemic opioids, or epidural anesthesia vs systemic). The Table summarizes the advantages and disadvantages of the 2 main surgical approaches for performing a uterotomy. For a fast and easy delivery of the puppies and minimal short- and long-term side effects for the bitch, we prefer the technique involving several openings at the level of the great curvature of each uterine horn rather than using only 1 opening at the level of the uterine body. Our technique is described later in Step 5 of the surgical procedure.
Procedure Pearl
Phenothiazines, barbiturates, ketamine, and atropine can all pass through the placenta and can affect the ability of neonates to thrive. Ideally, they should not be used.
Advantages & Disadvantages of Uterotomy Techniques
Advantages of Single Incision into Uterine Body
One incision
If few puppies, they are often easy to "milk" caudally into a single uterine incision
Disadvantages of Single Incision into Uterine Body
Uterine bleeding, resulting in increased risk for postsurgical adhesions with the bladder, colon, rectum
Potentially increased risk for postsurgical urinary incontinence, intestinal troubles, and risk for complications during future pregnancy
Weak scar tissue, resulting in:
reduced ability to contract during subsequent pregnancy
possible recurrence of dystocia
uterine rupture
Access to fetuses is more difficult:
if fetuses are numerous, increased risk for prolonged anoxia and early placental detachments
increased risk for puppy death
increased risk for bacterial contamination and tissue damage
Risk for intercornual septum rupture and bleeding
Longer duration of procedure if many puppies
Advantages of Multiple Uterine Horn Incisions
Incisions on the poorly vascularized great curvature of the uterine horns result in no bleeding; therefore reduced risk for postsurgical adhesions and, if any, major organs will not be involved (in most cases only the omentum)
Scar tissue does not involve any large muscle; therefore it has no effect on potential future contractions: natural whelping for future pregnancy is possible
Quick access to every fetus; therefore minimal stress for each and reduced risk for placental detachment and anoxia
Quick procedure if surgeon is well trained (less than 1 minute per puppy)
No extensive manipulation of the uterus; thus reduced risk for infection
Disadvantages of Multiple Uterine Horn Incisions
Multiple incisions require multiple sutures
Impossible to remove puppies from 1 horn through an incision made in the other due to a high risk for rupture of the intercornual septum
Increased closure time may negate, for the mother, the advantage of faster removal of puppies
Numerous incisions for potential dehiscence
Numerous potential sites for cicatricial lesions, adhesions
Step-by-Step: Cesarean Section in the Dog
Step 1: Administering the Anesthetic
Before making the incision, administer a local midline block. Inject lidocaine (0.5% to 1%, without epinephrine and after dilution with sterile water or normal saline), IM and SC along the incision line. (This may also be done in the preparation room if there is adequate time, which significantly reduces anesthesia duration.) Never exceed a total dose of 10 mg/kg of body weight. Lidocaine provides necessary analgesia during the initial steps of surgery. If used, opioids should be administered only after delivery of the puppies, thus reducing potential neonate depression. Readministration of long-acting local anesthetic can be used at closure, minimizing need for opioids.
Author Insight
Fluoroquinolones should never be used because of their negative effects on neonatal development and growth.

Step 2: Use of Antibiotics
A one-time preoperative IV injection of antibiotics may also be administered before induction, using a broad-spectrum cephalosporin. However, it is generally not needed, particularly for an elective c-section where there is no abnormality in the general condition of the bitch and no infection of the uterus. Fluoroquinolones should never be used because of their negative effects on neonatal development and growth.
Step 3: Opening the Abdomen
The recommended surgical approach for a c-section starts with a ventral midline incision from around the umbilicus to the cranial part of the pelvis. Puncture the very thin linea alba, taking care not to incise underlying organs. Continue the incision with blunt-tip scissors.

Step 4: Exteriorizing the Uterus
The highly dilated uterus is extremely fragile and presents a significant risk for rupture. Manipulate the uterus gently. To improve relaxation of ovarian pedicles and facilitate exteriorization of the uterus, apply 0.5 to 2 ml of lidocaine to the ovarian suspensory ligaments, which also dramatically reduces postoperative pain potentially associated with traction on the pedicles. Moreover, traction on ovarian pedicles may induce a vagal reflex, leading to hypotension and bradycardia; lidocaine helps prevent such a reflex. Locate and exteriorize tips of uterine horns.
Author Insight
Traction on ovarian pedicles may induce a vagal reflex, leading to hypotension and bradycardia; lidocaine helps prevent such a reflex.


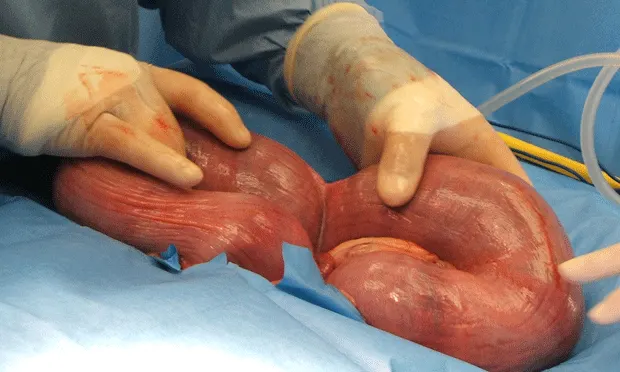
Step 5: Opening the uterus
Identify the individual fetuses and their placentas (A). Incise the uterine horns at the level of the great curvature and between 2 placentas (blue arrows) where the vasculature is minimal (yellow arrows). Puncture the horn with a bistoury blade (#10), and then extend the incision using blunt scissors (B) to prevent injury to the puppies.
The location of the incision allows rapid removal of 2 puppies or more. The cranial intercornual septum prevents a puppy located in the opposite horn or in the uterine body from being exteriorized through the contralateral incision. The rupture of the intercornual septum (directing puppies to the uterine body during whelping) can cause serious hemorrhaging. Always make an extra opening rather than lose time or risk contamination or rupture of the uterus by trying to remove all fetuses from a single opening. The number of openings will depend on the number and size of fetuses. It is most often 2 or 3.


Step 6: Delivering the Puppies
After locating the puppies, grasp the closest one either by the head or by the hindlegs (A). Open the fetal envelope with fingers (B & C) or scissors; envelopes can also be ruptured with a gauze sponge. Exteriorize the puppy; it is still connected to the uterus and oxygenated by the placenta through the umbilical cord. Wipe the nasal area.
Using 2 mosquito clamps, close the umbilical cord distal to the abdominal wall, and then cut between the 2 clamps (D). Give the puppy to the nursing team, who will take care of its complete resuscitation and homeostatic balance. Ideally the nursing team should include at least one person per pup. Leave the placenta in situ; all placentas will be removed after the delivery of the last fetus. This prevents anoxia, which is potentially observed when the placenta is separated at the time of fetus exteriorization (procedure whereby the whole fetoplacental unit is exteriorized and removed).
Repeat the procedure for all fetuses, making as many incisions as needed in the first and then second horn of the uterus. Puppies implanted in the body of the uterus are generally delivered using the most caudal incision.




Author Insight
Always make an extra opening rather than lose time or risk contamination or rupture of the uterus by trying to remove all fetuses from a single opening.
Step 7: Removing the Placentas
Once all fetuses have been delivered, the placentas are classically extracted. To separate a placenta, grasp the mosquito forceps still in place on the maternal side of the umbilical cord and gently pull the placenta to separate it from the uterus (A). The fetal placenta is characterized by its belt shape and the presence of 2 marginal hematomas (B), where the dark green uterine pigment, uteroverdine, is concentrated.
It is critical that the placental detachment occur between the fetal part of the placenta (trophoblast) and the endometrial part (C). If both layers of placental tissue are removed, there will be no uterine mucosa (endometrium) remaining; and an ovariohysterectomy may become necessary.
To assist in placental detachment, it is sometimes necessary to use one finger positioned between the fetal placenta and the uterus while simultaneously exerting gentle traction on the cord (C). Repeat the detachment procedure for all placentas.



Remove or Leave in Place?
Placentas are easy to detach when the c-section is performed at the expected due date (emergency c-section for a dystocia or perfectly timed elective c-section) but may be more difficult in preterm animals. Similarly, bleeding from the maternal endometrium is not a great concern when the c-section is perfectly timed, but it can be profuse if the surgery is performed too early. For this reason, difficult-to-detach placentas are more and more often left in situ to be expelled naturally during the next few days or resorbed.
Step 8: Closing Uterus & Abdomen
Inspect the uterus for lesions, ruptures, and hemorrhage. Collect bacteriologic swabs to check for potential bacterial infection when warranted (eg, stillborn fetuses, abnormal uterine content, etc).
Close the uterine incisions using a continuous inverted pattern (A) (Cushing or Lambert), with a 3-0 or 4-0 absorbable material (PDS, Vicryl; Ethicon, www.ethicon.com) on a taper-point needle. The suture should pass through the myometrium and submucosa, but should not be visible in the lumen of the uterus (it doesn't cross the entire endometrium). It is critical to tighten properly to make it as hermetic as possible. Having an assistant hold the uterus is a great help.
After closing the incisions, inject oxytocin, 1 to 5 (maximum) IU IV per dog. Check uterine contractility and incision sites for possible leakage. If the uterine sutures are leaking, a second tight continuous inverted pattern suture can be placed on top of the previous one. If a Cushing pattern has been used first, the second suture should be a Lambert pattern and vice versa.
Wash the uterus with physiologic saline to remove all blood clots, fibrin, and uteroverdine, which can promote the development of adhesions with the omentum (B). If the abdomen has been contaminated by fetal fluid (which generally happens), flush it with warm saline before replacing the uterus.
Close the abdomen routinely. Ideally the skin incision should be closed using an intradermal continuous pattern with 3-0 or 4-0 absorbable material. Any other kind of skin suture (staples, interrupted stitches, etc) can be susceptible to sucking by puppies, which can be a source of postoperative complications (dehiscence or infection). Do not puncture the mammary glands during closure.


Oxytocin
In an animal undergoing a c-section because of obstructive dystocia, uterine contractions have been ongoing for a long period prior to surgery; in such cases, the uterus may not be able to contract after the oxytocin injection. A second injection (same dose) is administered; higher doses of oxytocin are never recommended as they induce paralytic contraction of the uterus and desensitization of the receptors. If there is still no contraction, an ovariohysterectomy should be considered to prevent complications related to poor or absent uterine involution. Ovariohysterectomy done at this time does not affect milk production or release and will not prevent normal maternal behavior and nursing.
After the Procedure
Ideally, the dam will be totally awake soon after the procedure. She and her offspring should be returned to their natural environment as quickly as possible to facilitate establishment of the neonatal/maternal bond. Being in the comfort of their own environment reduces postoperative stress and mediates associated behavioral and lactation problems. For pain, NSAIDs and drugs like tramadol are always preferred to opioids, which are often associated with depression, hypothermia, and modified maternal behavior.