Brachycephalic Syndrome: Innovative Surgical Techniques
Laurent Findji, DMV, MS, MRCVS, DECVS, RCC Veterinary Referrals
Gilles Dupré, DMV, DECVS, University of Veterinary Medicine, Vienna, Austria
Canine brachycephalic syndrome (BS) consists of anatomic abnormalities (eg, stenotic nares, tortuous nasal cavities, aberrant conchae, elongated soft palate [ESP], everted laryngeal saccules, laryngeal collapse, tracheal hypoplasia) of brachycephalic dogs, which can lead to obstructive dyspnea and digestive disorders. In one study, 97% of brachycephalic dogs presented for BS had concurrent GI diseases.1 Upper obstructions (eg, nares, conchae, soft palate) may aggravate and sometimes cause deeper obstructions (eg, laryngeal, tracheal, bronchial collapses) and digestive disorders.
Early surgical correction of these abnormalities is often recommended and commonly includes treatment for stenotic nares and ESP. Other abnormalities (eg, laryngeal collapse2) occasionally require surgical attention but rarely in first intention. ESP, the most consistent anatomic abnormality encountered in dogs with BS, has been reported in up to 100% of cases.3,4 Initially, ESP was primarily described as excessive soft palate length, which can cause obstruction of the rima glottidis on inspiration (laryngeal obstruction). However, in many brachycephalic dogs, it has long been observed5-11 and recently demonstrated12,13 that the soft palate is also excessively thick, adding nasopharyngeal and oropharyngeal components to airway obstruction.
Folded flap palatoplasty (FFP) was developed to address the three components of obstruction caused by the soft palate by making it both thinner and shorter.8,9-11 Stenotic nares, when present, should be corrected following FFP. Various techniques have been described, but the authors prefer vertical wedge alaplasty, which consists of excising a vertical wedge from the ala nasi.
Comparing Traditional & Innovative
Conventional surgical techniques for eSP correction often consist of a simple resection of the redundant portion of the soft palate using different devices and various resection landmarks; although these techniques address the laryngeal component of obstruction, they may fail to fully address nasopharyngeal and oropharyngeal obstructions.14-26 FFP can address all components of the obstruction by reducing the soft palate’s length and thickness. The use of bipolar cautery in FFP increases intraoperative comfort. Compared with conventional staphylectomies, the suture material is more rostral and therefore farther from the pharynx, which should result in less postoperative pharyngeal inflammation and edema. Also, the rostroventral traction exerted on the remainder of the soft palate tends to further widen the nasopharyngeal opening. FFP tends to be longer and more technically demanding than conventional staphylectomy.
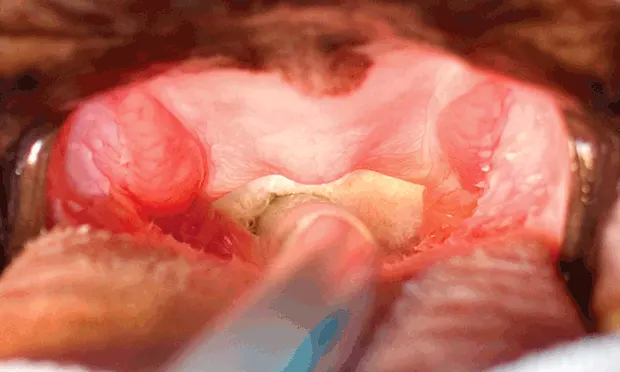
Before surgery, the patient should be premedicated (see Premedications to Consider) and stress avoided. Before anesthesia induction, oxygen can be supplied by mask or flow-by. Induction must be swift to allow prompt control of the airway via tracheal intubation. The pharynx should be examined and the larynx assessed for signs of laryngeal collapse.
Premedications to Consider
Acepromazine (0.01–0.05 mg/kg IM, SC)
Dexamethasone (0.1–0.2 mg/kg IM, SC)
Opioid analgesic (eg, morphine or methadone, 0.2–0.5 mg/kg IM)
Glycopyrrolate (2–10 µg/kg IM)
Antiemetics & antacids (SC or IM, depending on drugs)
What You Will Need
Basic surgical kit
Long instruments to facilitate the procedure in small dogs with narrow pharynges (eg, pugs)
Electrocautery
Precise monopolar cautery used in cutting mode for the initial palatoplasty incision
Bipolar electrocautery to facilitate hemostasis during the dissection of the soft palate
Absorbable monofilament sutures on swaged round or tapercut needles, size 3-0–5-0
Step-by-Step: Folded Flap Palatoplasty

STEP 1.
Place the dog in sternal recumbency. Restrain the head with the mouth open and the tongue gently pulled and fixed rostrally (Figures A, B, C).
Step-by-Step: Vertical Wedge Alaplasty

STEP 1A.
Start incising with a #11 scalpel blade at the apex of the wedge, which is positioned slightly dorsolaterally to the dorsal limit of the slit-like opening of the stenotic naris (Figure A).
Author Insight: The degree of postoperative opening of the naris will be grossly proportional to the angle chosen.