Anemia in a Cat—Can You Identify Why?
An adult spayed mixed-breed cat presented with ataxia and chronic left hindlimb weakness.
History
In addition to hindlimb weakness and ataxia, muscle atrophy was evident and the cat had a several-month history of listlessness. Cythioate (Proban) had been previously used for flea control, but not in the 2 months before presentation. The cat was referred to University of Florida Small Animal Hospital for neurologic examination.
Examination
On initial examination, the cat had pale mucous membranes, tachypnea, and a rectal temperature of 104°F. Orthopedic examination revealed a probable ruptured anterior cruciate ligament in the left hindlimb. Neurologic examination revealed signs of multifocal disease, including diminished motor control and sensation in the tail, decreased superficial sensation on the right side of the body, and hyperactive anal reflex in addition to ataxia.
Diagnostic Findings
The cat had macrocytic normochromic anemia (Table below). The plasma appeared colorless on whole blood centrifugation in a microhematocrit tube. Erythrocyte morphology included moderate anisocytosis without polychromasia (Figure 1).
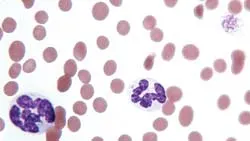
Figure 1 (View larger image). Giant hypersegmented neutrophil (left), normal-sized neutrophil (center), and macroplatelet (top right) in blood from a cat. Several macrocytic erythrocytes are also present. (Wright-Giemsa stain)
A platelet count was not done, but the platelet numbers appeared to be decreased (estimated 90 × 103/µL) on the stained blood film. Macroplatelets were often observed (Figures 1 and 2), along with lymphopenia and monocytosis. Occasional hypersegmented neutrophils and rare giant hypersegmented neutrophils were seen (Figures 1 and 3).
The serum biochemical panel was unremarkable. Because acetylcholinesterase activity was normal, organophosphate toxicity was considered unlikely.
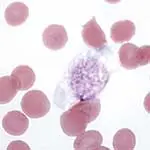
Figure 2 (View larger image). Macroplatelet (center) in blood from a cat. The granules appear as a pseudonucleus in the center of the platelet. (Wright-Giemsa stain)
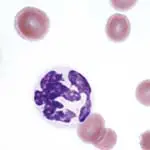
Figure 3 (View larger image). Hypersegmented neutrophil (bottom center) and macrocytic erythrocyte (top left) in blood from a cat. (Wright-Giemsa stain)
Findings Consistent with Macrocytic Normochromic Anemia
Ask Yourself…1. Is the anemia regenerative or nonregenerative?2. What is the general mechanism responsible for producing the anemia?3. What additional tests might you conduct to evaluate the anemia?
Diagnosis:
Myelodysplastic Syndrome (MDS)
Findings & Follow-Up Testing
The cat’s anemia appeared nonregenerative based on lack of polychromasia in the stained blood film. However, a reticulocyte count was not done to rule out the presence of increased punctate reticulocytes. Punctate reticulocytes, in contrast to aggregate reticulocytes, do not appear polychromatophilic in stained blood films. However, the clinician would expect increased numbers of aggregate reticulocytes to be released from the bone marrow in response to a hematocrit of 16%, assuming the anemia was present for at least 3 to 4 days (ie, the time required for the formation of aggregate reticulocytes in bone marrow).
Based on the history of listlessness for several months, anemia had likely been present for at least several weeks to months. The mean cell volume was slightly increased, indicating that increased anisocytosis may have resulted from macrocytic erythrocytes in the blood. Anisocytosis may be present in both regenerative and nonregenerative anemia. In this cat, nonregenerative anemia may have resulted from decreased erythrocyte production. Macrocytic platelets may be released in response to peripheral platelet utilization or destruction but have also been reported in animals with dysplastic megakaryocytopoiesis.
Lymphopenia, eosinopenia, and monocytosis may have resulted from endogenous glucocorticoid release. Neutrophilia is also expected in response to glucocorticoids; however, the neutrophil count tends to normalize with chronic glucocorticoid exposure. The presence of occasional hypersegmented and rare giant neutrophils in this patient suggested that dysgranulopoiesis may have been present in the bone marrow.
Macrocytic nonregenerative anemia is common in FeLV-infected cats, and the FeLV test was positive in this cat. Nonregenerative anemia with thrombocytopenia and/or leukopenia may also occur with feline immunodeficiency virus (FIV) infection; however, this test was not conducted and a combined infection cannot be ruled out. However, once MDS was diagnosed, the case workup, including more sophisticated neurologic examination, was curtailed.
Because the presence of nonregenerative anemia, thrombocytopenia, and neutrophilic morphologic abnormalities suggested a bone marrow disorder, a bone marrow aspirate was obtained.
Related Article: Coombs Testing: A Diagnostic Step for Anemic Cats
Aspiration Findings
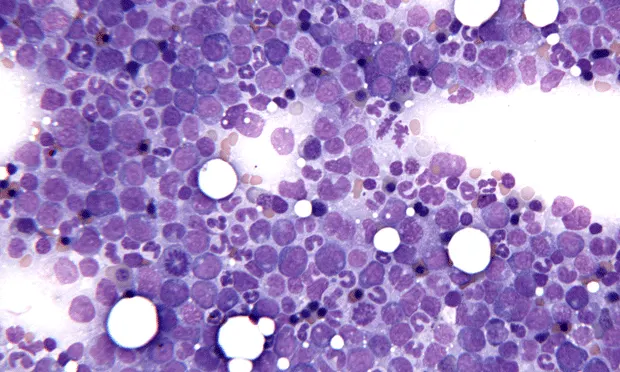
The bone marrow was of normal or increased cellularity (Figure 4). Megakaryocytes were present in normal numbers, but abnormal dwarf megakaryocytes were also observed (Figure 5).
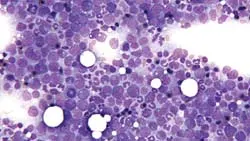
Figure 4 (View larger image). Cellular bone marrow aspirate smear from a cat with a left shift in the granulocytic series, increased mitotic figures, and megaloblastic erythroid precursors. (Wright-Giemsa stain)
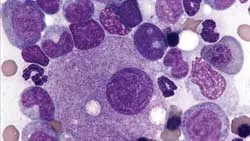
Figure 5 (View larger image). Dwarf megakaryocyte (center) and megaloblastic erythroid precursor (top right) in a bone marrow aspirate smear from a cat. (Wright-Giemsa stain)
Both the erythroid and myeloid series were complete, but both series had morphologic abnormalities. Erythroid cells were often megaloblastic (Figure 6), with a moderate increase in immature cell types. The myeloid series had an increased proportion of cells in the proliferating pool (ie, myeloblasts, promyelocytes, myelocytes) relative to cells in the maturation and storage pool (ie, metamyelocytes, bands, mature neutrophils). Myeloblasts accounted for less than 5% of all nucleated cells.
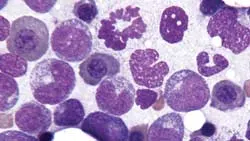
Figure 6 (View larger image). Three megaloblastic erythroid precursors (across top half of image) and 2 mitotic neutrophil precursors in a bone marrow aspirate smear from a cat. (Wright-Giemsa stain)
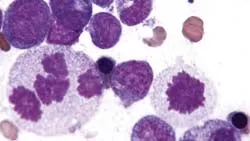
Figure 7 (View larger image). Three mitotic neutrophil precursors in a bone marrow aspirate smear from a cat. One large neutrophilic precursor (left) contains 4 mitotic figures. (Wright-Giemsa stain)
Mitotic granulocytic cells were increased, and occasional giant neutrophilic cells and abnormal mitotic figures were recognized (Figure 7). The myeloid-to-erythroid (M:E) ratio was 1.7 (range, 1.2–2.2).
Did You Answer...1. Nonregenerative2. Decreased erythrocyte production3. FeLV/FIV tests and bone marrow biopsy
Discussion
Myelodysplasia
The term myelodysplastic syndrome is generally used as a synonym for primary myelodysplasia. MDS consists of a heterogenous group of neoplastic disorders that are characterized by peripheral cytopenias, especially nonregenerative anemia and thrombocytopenia, with normal to hypercellular, dysplastic-appearing bone marrow. This ineffective hematopoiesis results from defective maturation and extensive apoptosis (physiologic cell death) of hematopoietic cells.
As with MDS in humans, a clonal proliferation of hematopoietic cells has been identified in two-thirds of cats with MDS, suggesting that MDS may be considered a preleukemic state for acute myeloid leukemia (AML) in cats. FeLV (and probably FIV) infections can produce MDS in cats, although some cats with MDS may have negative test results for these viruses.
As observed in this case, evidence of dyserythropoiesis, dysgranulopoiesis, and/or dysmegakaryocytopoiesis is present in the marrow of animals with MDS. Additional abnormalities may include: nonregenerative anemia with erythrocyte macrocytosis, anisocytosis, and/or poikilocytosis; nucleated erythrocytes (metarubricytosis) out of proportion to the number of reticulocytes present; nucleated erythrocytes with lobulated or fragmented nuclei; thrombocytopenia; and large bizarre platelets, immature granulocytes, and abnormal granulocyte morphology.
Types of Myelodysplastic Syndrome
MDS has been classified into 3 subtypes in animals: MDS with erythroid predominance in the bone marrow (M:E ratio <1) may be classified as MDS-erythroid (MDS-Er). Cases with refractory anemia and an M:E ratio >1, with or without other refractory cytopenias, may be described as MDS-refractory cytopenia (MDS-RC). Myeloblasts account for less than 5% of all nucleated cells in this subtype. When myeloblasts are increased (5%–19% of bone marrow nucleated cells), the term MDS-excess blasts (MDS-EB) may be used.
This cat can be classified as MDS-RC because the M:E ratio was >1.0 and myeloblasts did not exceed 5% of all nucleated cells. Cats with MDS may subsequently develop AML, and FeLV-positive cats with MDS have reportedly developed lymphoid neoplasms.
MDS must be differentiated from secondary myelodysplasia, which may be associated with immune-mediated disorders (immune-mediated hemolytic anemia, immune-mediated thrombocytopenia), lymphoid neoplasms, myelofibrosis, drugs that interfere with DNA synthesis, heavy metal toxicity, certain antibiotics, and anticonvulsant drugs. Once the client learned that the cat was FeLV positive with MDS, the decision was not to pursue further diagnostic evaluation for ataxia. The cat was released on palliative therapy and lost to follow-up.
AML = acute myeloid leukemia, MDS = myelodysplastic syndrome, MDS-EB = MDS-excess blasts, MDS-Er = MDS-erythroid, MDS-RC = MDS-refractory cytopenia, MCV = mean cell volume, MCHC = mean cell hemoglobin concentration
For related articles, please see the following:What Type of Anemia?Hemolytic Anemia in a CatWeight Loss, Polyphagia, & Ataxia in a Cat