Iris Nodule in a Cat
Alexandra van der Woerdt, DVM, MS, Diplomate ACVO & ECVO, Animal Medical Center, New York, New York
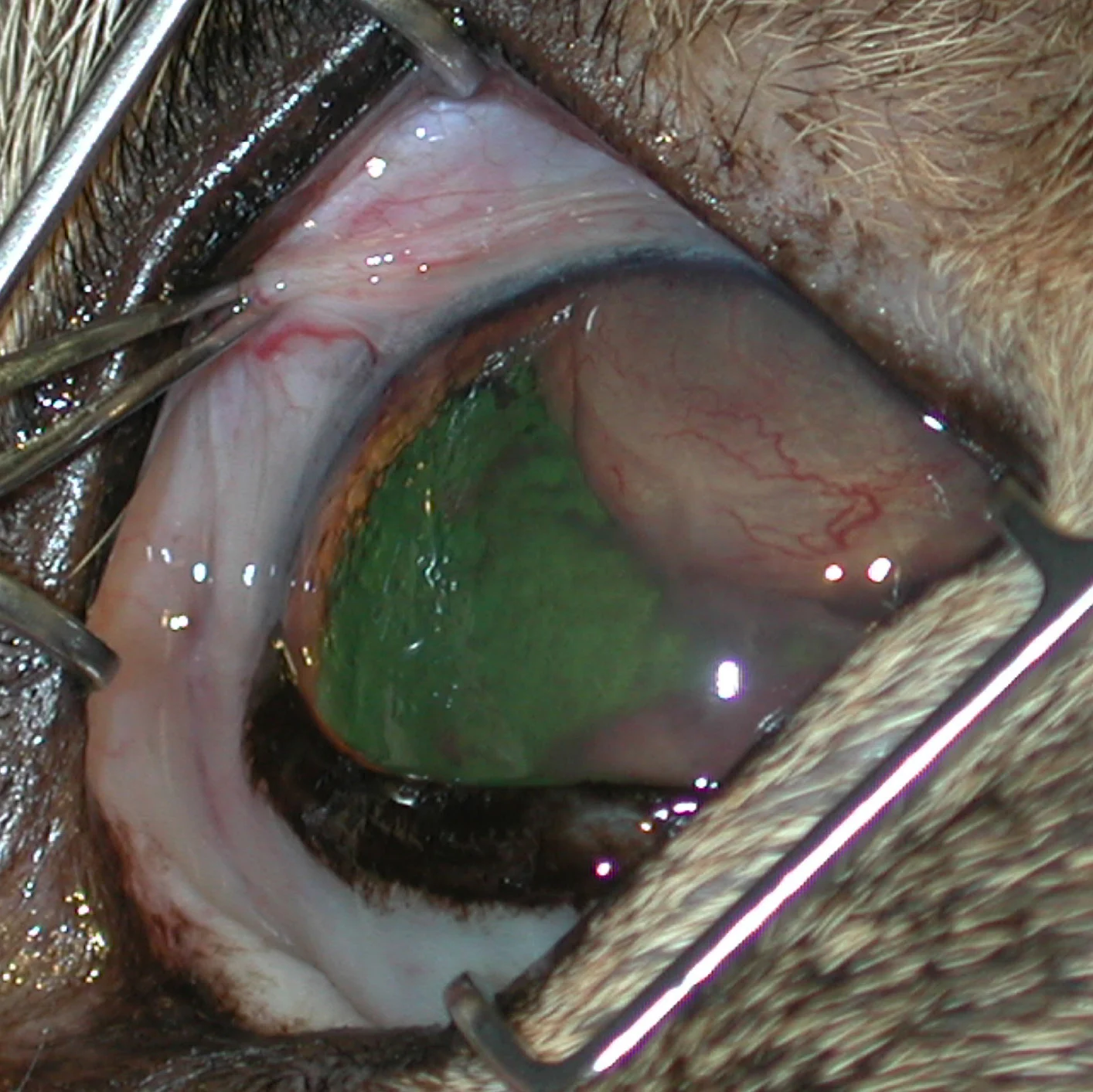
The left eye of a cat presented for evaluation of an iris nodule. Note the raised, vascular, pink mass associated with the lateral part of the iris.

Concentrated preparation of aqueous humor. A few scattered red blood cells and nondegenerate neutrophils are present. Approximately 70% to 80% of the nucleated cells are tissue cells consisting of large, irregular round cells. (Wright-Giemsa stain; original magnification, 400×)
A neutered male domestic shorthair cat, which was approximately 15 years old, was presented for evaluation of an iris nodule in the left eye.
History
The owner first noticed the abnormality 1 week before presentation. Anterior uveitis was diagnosed by the referring veterinarian. Blood was submitted for a CBC, biochemistry profile, serum T4 concentration and FeLV antigen (ELISA), FIV antibody, feline coronavirus (IFA), and Toxoplasma gondii IgG and IgM antibody titers. Urine was submitted for urinalysis. Treatment was started using oral amoxicillin/clavulanic acid and topical gentamicin ophthalmic solution. The cat was referred to the Animal Medical Center for evaluation when the mass seemed to enlarge despite therapy.
Ophthalmic Examination
Slit-lamp biomicroscopy and indirect ophthalmoscopy were used for the examination. No significant abnormalities were found in the right eye. The left eye had a weak menace response and a slow pupillary light reflex. Mild aqueous flare and a clot of fibrin with red blood cells were present in the anterior chamber. In the lateral part of the iris, a pink vascular mass protruded into the anterior chamber (Figure 1). Vitreal infiltrates precluded detailed examination of the fundus. The systolic blood pressure was measured using a noninvasive Doppler technique and was judged to be at the upper end of normal at 160 mm Hg.
Laboratory Analysis
Abnormalities revealed in the laboratory analysis are given in the Table. All submitted titers were negative; the T4 was within normal limits; and urinalysis was unremarkable with a urine specific gravity of 1.058.
Diagnostic Testing
Anterior chamber aspiration was determined to be the next diagnostic step. The cat was anesthetized with intravenous propofol and diazepam, intubated, and maintained on oxygen for the short duration of the procedure. Several drops of 0.5% proparacaine ophthalmic solution were applied a few minutes apart to the eye. One quarter of a milliliter of aqueous humor was slowly withdrawn from the anterior chamber by using a tuberculin syringe with a 25-gauge needle inserted at the limbus of the eye. The sample was submitted for cytologic evaluation. Figure 2 shows a centrifuged preparation of the aqueous humor sample.
Ask Yourself...
What is the most likely cytologic diagnosis?
Which other differential diagnoses were you considering before the anterior chamber aspiration?
Diagnosis:
Malignant round cell neoplasm-most consistent with atypical, extranodal lymphoproliferative disease

Note the large round cells (thick arrow), mitotic figure (thinner arrow), and multiple nucleoli (thinnest arrow). (Wright-Giemsa stain; original magnification, 400×)

Concentrated preparation of aqueous humor. Note the intracytoplasmic spherical granules (thick arrow). Small amounts of melanin pigment granules are present (thin arrow). (Wright-Giemsa stain; original magnification, 1000×)
Cytology
The tissue cells consist of large, irregular round cells with a fine to slightly coarse nuclear chromatin pattern. Prominent, sometimes irregular and sometimes multiple, nucleoli are present (Figure 2). Most of the intact cells contain indented-to-ameboid-shaped nuclei with variably abundant light-staining cytoplasm. Some contain small, slightly basophilic to metachromatic spherical granules (Figure 3). Occasional bizarre mitotic figures are observed, and a few small lymphocytes are also seen.
The presence of these intracytoplasmic granules may be consistent with lymphoma of the large granular lymphocytic variety. This form of lymphoproliferative disease generally originates from the abdominal cavity.
Additional Diagnostics
Additional diagnostic tests, including chest and abdominal radiographs and abdominal ultrasonography, were recommended but declined by the owner.
Did You Answer...
Malignant round cell neoplasm
Inflammatory nodule versus other neoplastic diseases, such as amelanotic melanoma
Discussion
Ocular involvement in multicentric lymphoma is common in dogs and cats.1 In one study, ocular changes consistent with systemic lymphoma were present in 37% of dogs examined.1 Ocular lymphosarcoma can initially present as anterior uveitis in cats.2,3 Nonspecific lymphocytic-plasmacytic uveitis (diffuse or nodular) was the most common type of uveitis in a large retrospective histopathologic study of uveitis in cats .3 Lymphosarcoma was also common, affecting 24% of globes in the study.
In a retrospective study evaluating histopathologic features of feline ocular lymphosarcoma, inflammation was present in 50% of eyes studied.2 Lymphosarcoma was nodular (as in the case presented here) in 70% of eyes and diffuse in 20% of eyes. Secondary complications, such as glaucoma or retinal detachment, are common.
The intracytoplasmic granules noted in the sample obtained from this cat are highly suggestive of lymphoma of the large granular lymphocytic variety, originating in the abdominal cavity.4 Low levels of serum albumin, which is present in this case, can be present in cats with intestinal lymphosarcoma. Treatment of ocular lymphosarcoma is best done by treatment of the lymphosarcoma elsewhere in the body.5 Ocular lymphosarcoma can respond dramatically to chemotherapy, and enucleation is generally not necessary.
Aqueocentesis with subsequent cytologic evaluation of a centrifuged preparation of aqueous humor enabled us to differentiate between chronic inflammatory changes and neoplastic disease.6 It also allowed us to determine whether the eye needed to be removed (which would be the case in neoplastic diseases other than lymphosarcoma) or whether the eye could be spared and treated with chemotherapeutic agents.
Acknowledgment
The author thanks Andrew Loar, DVM, Diplomate ACVIM, for his assistance with the manuscript.