Chronic Keratoconjunctivitis in a Cat
David J. Maggs, BVSc (Hons), DACVO, University of California, Davis
History
The cat lives with two other cats, neither of which has ocular signs. The cat was seen 5 weeks ago by another veterinarian for unilateral mucopurulent ocular discharge. The veterinarian applied fluorescein stain, diagnosed an ulcer, and prescribed neomycin-polymyxinbacitracin ophthalmic ointment to be applied to the affected eye three times daily. After 7 days, there was incomplete improvement. Subsequent treatments have included atropine ophthalmic ointment once daily for 7 days and then combined antibiotic-steroid (neomycin-polymyxin-bacitracin-hydrocortisone) ointment three times daily for a week when fluorescein stain was no longer retained by the cornea. The cat has received trifluridine (antiviral) ophthalmic solution twice daily for the last week. The owners report no other health concerns. The cat behaves as if sighted.
Physical Examination
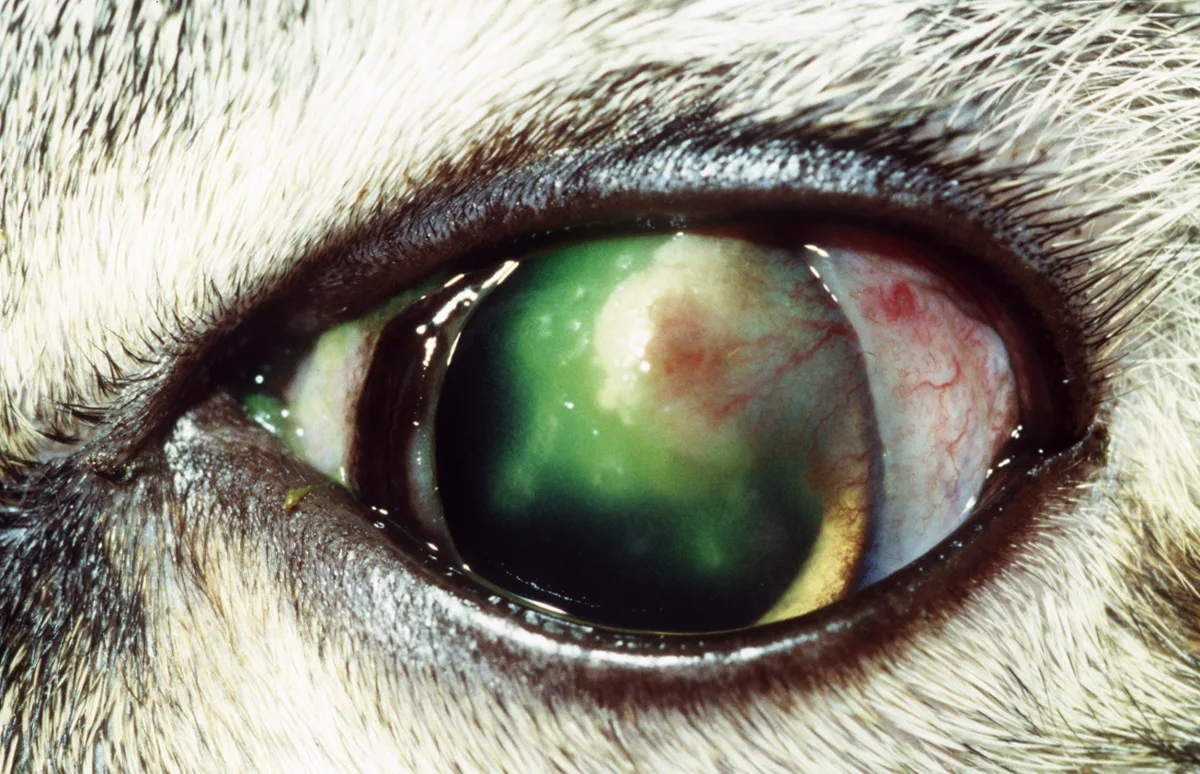
No abnormalities were noted on general physical examination. The right eye was normal. Mild blepharospasm was noted in the left eye (Figure 1). Pupillary light reflexes were normal; a Schirmer's tear test revealed wetting of 12 mm/min in the left eye and 8 mm/min in the right eye; and intraocular pressure as measured with a Tono-pen (Medtronic Solan, Jacksonville, FL) was 13 mm Hg in both eyes. Fluorescein stain was applied to the eye, and the pupil was dilated for subsequent fundic examination. No abnormalities were noted on intraocular or fundic examination.
Ask Yourself...
Describe the cat's ocular lesions as fully as possible.
What is the most common cause of keratoconjunctivitis in cats?
Does lack of response to trifluridine applied twice daily rule out FHV-1?
What diagnostic test is likely to be most useful in this cat?
Diagnosis:
Feline proliferative (eosinophilic) keratoconjunctivitis
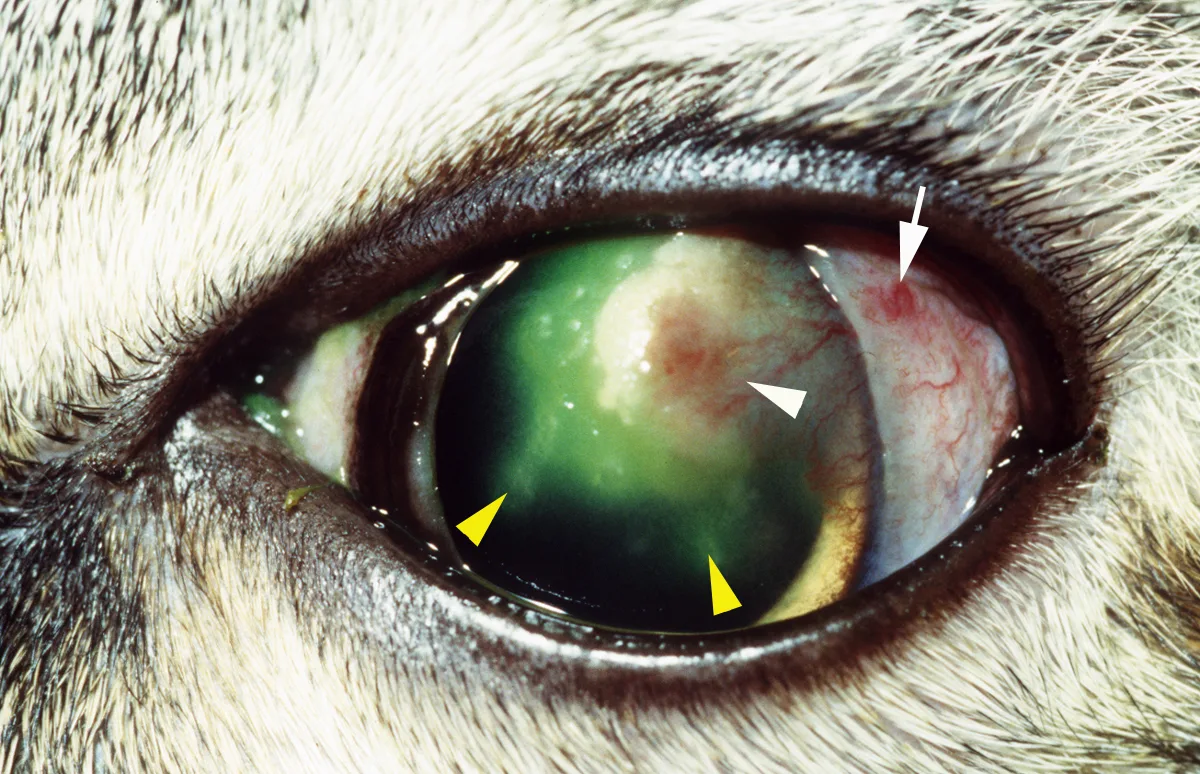
Examination of the left eye (Figure 2) reveals a small amount of mucoserous discharge visible at the medial canthus and moderate bulbar conjunctival hyperemia laterally, with some vessels forming a slightly raised meshwork of capillaries (white arrow). The lateral cornea has a coalescing series of slightly raised, yellow plaques and superficial vascularization (white arrowhead). Fluorescein has been retained by the cornea axial to the plaques, including two small, linear regions projecting further axially (yellow arrowheads), suggestive of dendritic (herpetic) ulcers. The clinical diagnosis is proliferative and ulcerative keratoconjunctivitis.
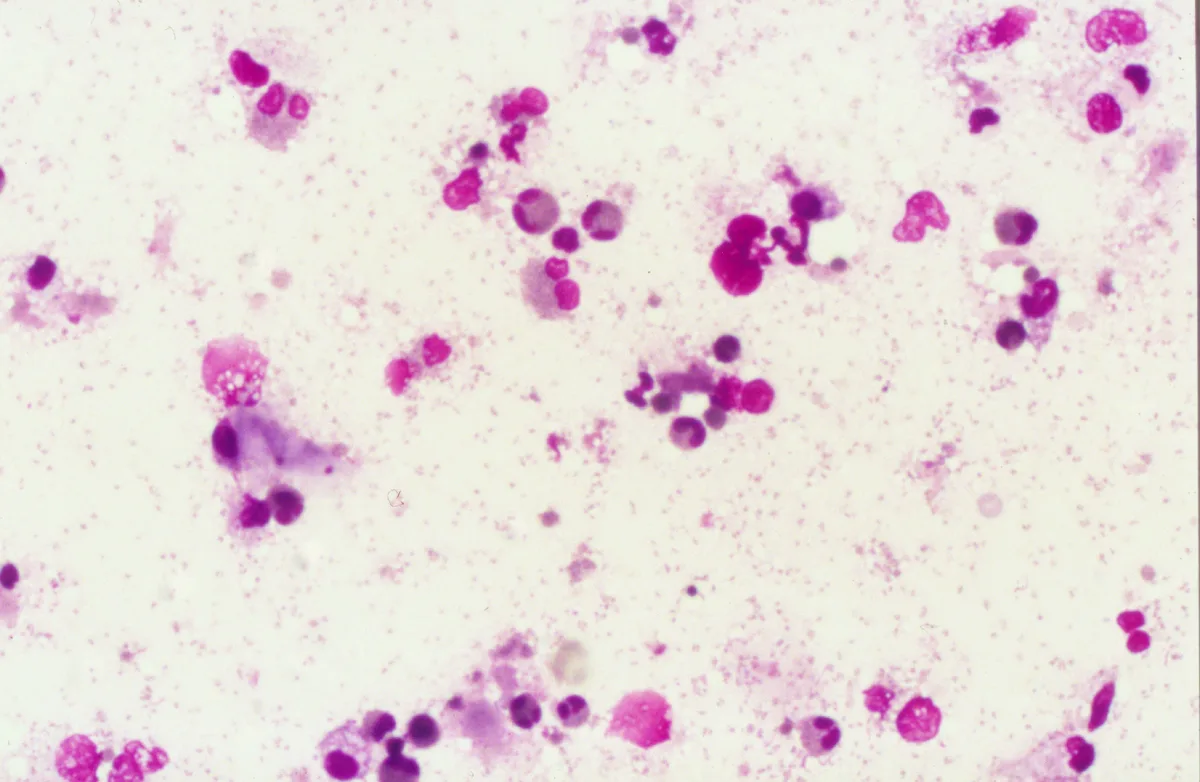
Cytologic assessment is the diagnostic test of choice whenever raised lesions are found on the cornea and/or conjunctiva. Assessment can be done in many cases with only topical anesthesia and the base of a sterile scalpel blade. On this occasion, the plaques felt gritty when scraped and cells exfoliated readily; when examined microscopically, the cells were a mixed population of white blood cells and epithelial cells. Abundant eosinophils were seen (Figure 3).
Proliferative keratoconjunctivitis appears as focal, raised plaques, sometimes with adjacent ulceration. It typically involves the lateral cornea. Eyelid or conjunctival involvement is relatively common, and occasionally these surface structures are affected in the absence of keratitis. Diagn
osis is suggested by clinical appearance and confirmed when eosinophils are seen on cytologic evaluation.
The condition is probably an aberrant immune response. FHV-1 DNA can be detected in corneal samples from approximately 75% of cats with proliferative keratoconjunctivitis, leading some to incriminate the virus. Proliferative keratoconjunctivitis has traditionally been treated with topical corticosteroids; however, the presence of corneal ulcers and involvement of FHV-1 present a dilemma. Some patients may improve on antiviral medications alone, especially if administered at least 4 to 6 times daily. However, immunomodulatory therapy (topical corticosteroids or occasionally-and with adequate informed client consent-systemic megestrol acetate) is usually also required. Recurrence is common, but early diagnosis and treatment of recurrent episodes limit the need for protracted therapy. Figure 4 shows the appearance of this cat after 3 weeks of treatment.

Did You Answer...
This cat has keratoconjunctivitis. The corneal lesions are both plaque-like (proliferative) and erosive (ulcerative). A full description of all lesions is provided in the text.
FHV-1 is the most common cause of feline corneal and conjunctival disease. Chlamydophila felis (previously Chlamydia psittaci) is also a common cause of conjunctivitis-but not keratitis-in cats.
Because all topical antiviral agents are virostatic, they must be applied frequently (4 to 6 times daily) to be effective. Therefore, failure to respond to less-frequent application does not rule out FHV-1.
As with other plaque-like lesions, the most useful diagnostic test is cytologic examination of a sample harvested from affected tissue. This can be done safely on corneal and conjunctival plaques.
TX at a Glance
Topical antiviral agents, such as idoxuridine 4-6 times daily
Consider lysine 500 mg PO twice daily
Once ulceration is controlled, consider a penetrating topical corticosteroid, such as dexamethasone or prednisolone acetate 2-4 times daily