Proteinuria is the presence of increased concentration of protein in the urine. In a healthy kidney, the glomerular filtration barrier retains large proteins in the plasma (molecular weight, >68 kDa). Proteins with a molecular weight <68 kDa are freely filtered and resorbed in the proximal tubules so that the vast majority are not lost in urine1; however, trace to >1 protein on a urine dipstick is frequently seen in concentrated urine samples from healthy dogs.2 This phenomenon is not typical in healthy cats.2 Studies have shown that significant and persistent proteinuria in cats, dogs, and humans is highly correlated with reduced survival in azotemic and nonazotemic patients. Detection and management are thus important, as reduction in proteinuria has been shown to increase survival.1,3-5
A thorough diagnostic workup is critical. Localization of the cause and determination of persistence and magnitude of proteinuria are important factors. Proteinuria is persistent if >3 urinalysis tests are positive for significant protein over a period of ≥2 weeks. Quantification of proteinuria is often determined via urine protein:creatinine ratio (UPCR), which can also be used to assess response to treatment, as UPCR is increased in any patient with proteinuria.6 UPCR is most useful diagnostically when the sediment is inactive, meaning there is no evidence of inflammation, infection, or hemorrhage in the sediment, and overflow causes (ie, pathologic states that increase the plasma concentration in proteins small enough to pass through glomerular filtrate) have been ruled out.2
Following are the top 5 most common causes for proteinuria in dogs and cats according to the authors.
1. Inflammation of the Urinary Tract
UTIs are the most common cause of proteinuria. Bacterial cystitis and pyelonephritis typically occur via ascending bacterial infections. This type of proteinuria arises when plasma proteins leak through vessel walls, secondary to a local release of inflammatory cytokines. Hematuria and pyuria are expected findings on routine urinalysis.2 Fewer than 5 WBCs per high-power field (HPF) is considered within the reference interval, whereas an increased number of WBCs (≥5) is considered pyuria7,8; however, these values are based on sediment from 5 mL of urine. If only 1 mL of urine is evaluated, the expected WBC count per HPF would be 5 times fewer (ie, 1 WBC per HPF).9 Other potential causes for inflammation of the bladder include urolithiasis, neoplasia (eg, urothelial cell carcinoma [previously known as transitional cell carcinoma]), prostatitis, pyometra, vaginitis, and hemorrhagic cystitis.10 Obtaining a sample via cystocentesis can help determine whether inflammation is localized to the urinary bladder or originates from other areas of the lower urinary tract (eg, prostate, prepuce, uterus, vulva). An active urine sediment (ie, increased RBCs [hematuria], WBCs [pyuria], bacteriuria) (Figure 1) is expected in patients with inflammation.9

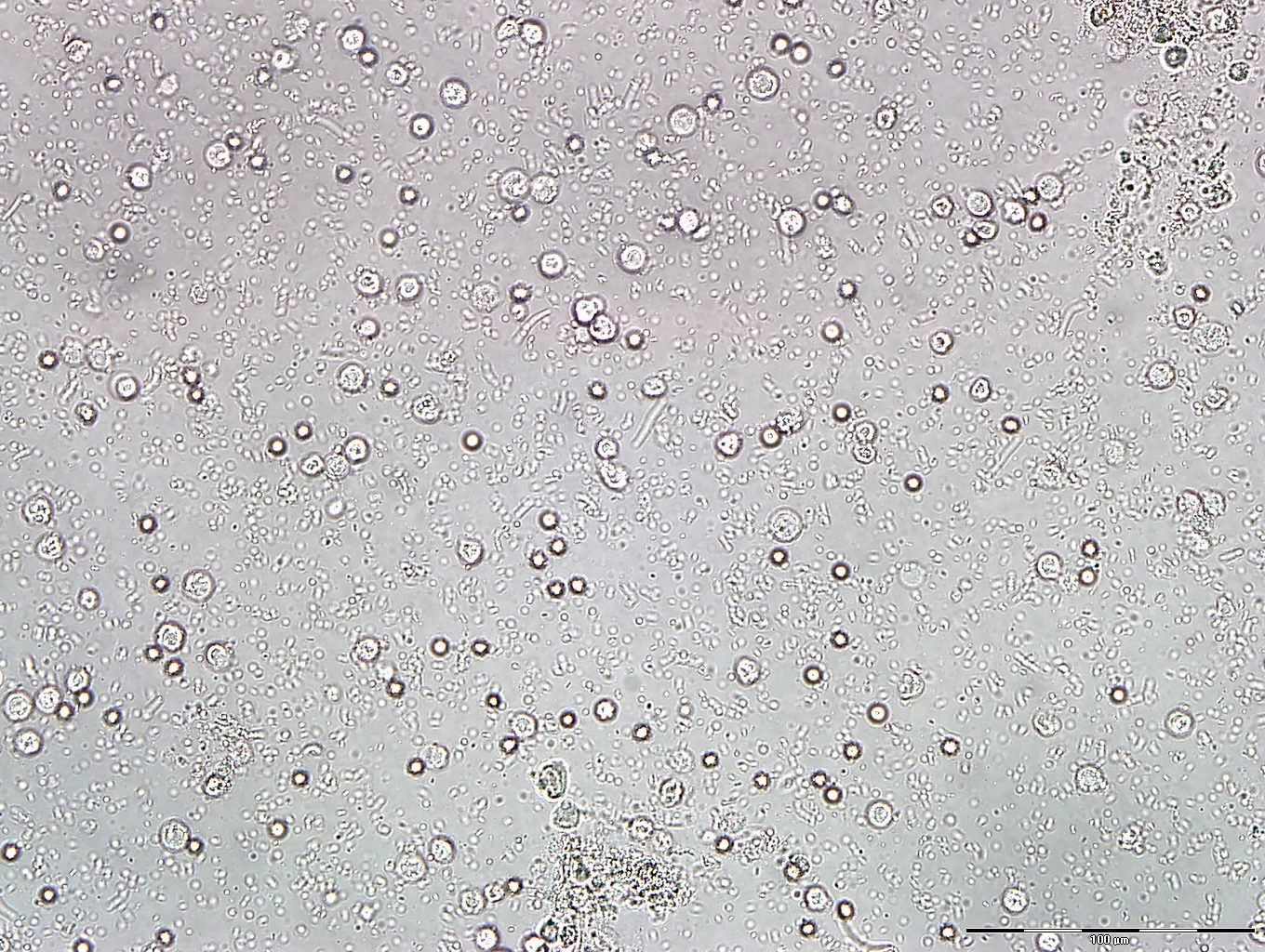
FIGURE 1 Unstained wet mount of urine sediment showing findings consistent with bacterial cystitis or pyelonephritis. WBCs (arrowheads) and RBCs (arrows) are present with abundant bacteria in the background.
Systemic inflammation may, at times, also result in inflammatory proteinuria. For example, in patients with pancreatitis or acute kidney injury with inflammation, proteinuria may occur secondary to renal microcirculation damage caused by hypovolemia, cytokine-induced ischemia, or oxidative stress. Patient history, physical examination, urinalysis, CBC, serum chemistry profile, and imaging must be correlated for diagnostic accuracy.11
2. Hemorrhage
Blood in the urine increases protein concentration due to added plasma proteins and, if erythrocytes have lysed, hemoglobin.2 Causes for hematuria (ie, hemorrhage into the urinary tract) (Figures 2 and 3) are numerous. The more common causes include lower urinary tract disease, urolithiasis, bacterial cystitis, and neoplasia. Inflammation and hemorrhage are often concurrent. Other possible differentials include blood vessel damage from trauma, neoplasia, necrosis, iatrogenic causes (eg, obtaining urine via cystocentesis or a catheter), impaired hemostasis, and idiopathic renal hematuria (rare; ie, benign essential hematuria). Potential causes for impaired hemostasis include anticoagulant intoxication, disseminated intravascular coagulation, hemophilia, hepatic failure, or thrombocytopenia.10,12

FIGURE 2 Unstained wet mount of urine sediment from a cat with feline lower urinary tract disease. Numerous RBCs (arrows) with fewer WBCs (arrowhead) are consistent with hemorrhage.

FIGURE 3 Comparison of 2 different fresh urine samples after centrifugation. Before centrifugation, both samples were red. Sample A contains red supernatant and few to no RBCs in the urine sediment, consistent with hemoglobinuria or myoglobinuria. With hemoglobinuria, plasma is also red, and the patient will be anemic. With myoglobinuria, clear plasma and increased muscle enzymes (eg, creatine kinase, aspartate aminotransferase) can be expected. Conditions like high urine pH (>8) or very low urine specific gravity (<1.006) may cause RBC lysis in the sample; interpretation should be correlated with clinical findings. Sample B looked similar to sample A before centrifugation; however, clearing of the red color via centrifugation and presence of RBCs in the sediment suggest that hematuria is the cause of the red urine.
A normal RBC concentration for voided urine is <5 RBCs per HPF (based on sediment from 5 mL of urine).9 If urine is obtained via cystocentesis or catheterization, RBC counts can be >100 per HPF, although the samples should still appear grossly yellow and lack proteinuria.1,7,8 Patients with proteinuria secondary to significant noniatrogenic hemorrhage will likely have macroscopic hematuria and active sediment with marked RBCs visible on microscopic examination.13 Follow-up to determine whether proteinuria resolves after treatment and/or management of the underlying cause is important. It has been shown hematuria and pyuria may not be the sole contributors to proteinuria, and underlying disease may remain undiagnosed.13
3. Glomerular Disease
Glomerular disease, sometimes referred to as protein-losing nephropathy, results from failure of the glomerular filtration barrier to retain larger, negatively charged proteins. Glomerular protein loss may range from mild to severe depending on disease stage. Mild protein loss (UPCR ratio <1) and absence of hypoalbuminemia and hypoproteinemia are possible early in disease progression. As protein loss increases, a selective hypoproteinemia (ie, loss of specific proteins like albumin and possibly globulins of similar size or slightly larger) results.2 If UPCR in a dog with inactive sediment is >2, glomerular disease should be considered1,6; however, lower UPCR does not rule out glomerular pathology. Further, with absence of hyperproteinemia and presence of an otherwise normal urinary tract (ie, inactive urine sediment), significant increases in protein in the urine (UPCR >5) indicates glomerular protein loss.2 In cats, UPCR >2 with concurrent inactive urine sediment should indicate high suspicion of glomerular disease. Persistent loss of protein via the glomerulus may also cause or contribute to tubular damage as the kidney attempts to resorb these excess lost proteins.1,4,14
Glomerular disease has many causes and is more common in dogs than in cats. Some differentials include amyloidosis, membranoproliferative glomerulonephritis secondary to various infectious and noninfectious causes (eg, Lyme disease, Ehrlichia spp, FeLV, FIP, FIV, neoplasia, immune-mediated disease), glomerulosclerosis (eg, secondary to systemic hypertension, hyperadrenocorticism), and renal maldevelopment.1,2 If UPCR is >20, acquired or reactive amyloidosis, glomerulosclerosis (ie, loss of podocytes, scarring secondary to chronic insult), and immune-complex–mediated glomerulonephritis should be considered.1,2,15 Amyloidosis can often result from genetic or familial causes, with certain breeds (eg, shar peis) predisposed.1
Azotemia may not be present with glomerular disease, especially early in the disease. Glomerular disease with persistent proteinuria indicates a form of chronic kidney disease, with some patients living a normal lifespan while others progress rapidly to kidney failure, depending on the cause of glomerular dysfunction.1,10 Protein loss may become significant as the disease progresses, and development of a selective hypoproteinemia may occur. Albumin is generally lost first, followed by loss of larger globulins (eg, antithrombin) and potentially resulting in a variety of systemic sequelae, including increased risk for thrombosis and nephrotic syndrome (characterized by hypoproteinemia, proteinuria, hypercholesterolemia, and edema or effusion).2
4. Tubular Disease
Proteinuria from tubular disease is a result of impaired tubular reabsorption of proteins normally filtered through the glomerulus. These proteins are freely filtered and are typically low to moderate (rare) molecular weight proteins (eg, albumin).2,6 The magnitude of proteinuria in patients with tubular disease is usually mild, with UPCR <2.2,9 Tubular disease is unlikely to lead to hypoproteinemia, as long as the remainder of the nephron is functioning normally.6 In cases in which the cause of proteinuria (glomerular vs tubular) is unclear, additional diagnostics via a referral laboratory (eg, sodium dodecyl sulfate-polyacrylamide gel electrophoresis [SDS-PAGE] testing) can be requested to determine the average size of the lost proteins.1,2
Differentials for tubular proteinuria include leptospirosis and exposure to common nephrotoxins (eg, ethylene glycol, grapes/raisins, lilies [cats], NSAIDs), which are toxic to the renal tubules and can lead to tubular necrosis and loss of protein in the urine, integrity, and resorptive ability.10,16 The degree of proteinuria has prognostic indications. Reports indicate that cats with UPCR >0.4 live ≈50% as long as those with UPCR <0.4.1
In addition, Fanconi syndrome is an inherited or occasionally acquired disease of the proximal renal tubules that leads to defects in the resorption of glucose, ketones, amino acids, phosphate, bicarbonate, calcium, and/or potassium, as well as various renal defects. Proteinuria is common in these patients, but results tend to indicate negative or only a mild increase in urine protein with standard urinalysis testing.9 As with glomerular disease, if protein loss is solely from tubule dysfunction, inactive sediment (ie, an absence of inflammation) would be expected on microscopic examination of urine.2,9
5. Overload Proteinuria
Overload (ie, overflow) proteinuria is a prerenal cause of proteinuria and occurs when a pathologic state causes an increase in plasma concentration of small proteins that are able to pass freely through a healthy glomerulus and are abundant enough to overwhelm the resorptive capacity of the renal tubules.2
Hemoglobin, myoglobin, and Bence Jones proteins are commonly associated with overload proteinuria. Hemoglobin from RBCs broken down via intravascular hemolysis can overwhelm the tubules and cause plasma and urine to appear pink or red. In patients with intravascular hemolysis, hemoglobinemia occurs before hemoglobinuria, and anemia will be present.2 Myoglobin from the breakdown of muscle fibers can cause proteinuria in a similar manner; however, plasma will appear normal (ie, clear and colorless), and urine may appear pink, red, or amber.2
Lastly, Bence Jones proteins are excess immunoglobin light chains produced as a result of neoplastic transformation of B cells or plasma cells and are subsequently excreted in the urine when the renal tubules are overwhelmed. Bence Jones proteins do not show an increased protein result on a urine dipstick unless present in high quantities.2 Inactive sediment can be expected if overload proteinuria is the cause.2
Conclusion
In cases in which proteinuria is noted on urinalysis, further investigation with strategic diagnostics to determine the underlying cause is important. Active sediment proteinuria like inflammation or hemorrhage are the most common causes. Persistent proteinuria with inactive sediment has significant prognostic implications in veterinary patients and warrants management and treatment strategies to limit progression.