Surgical Treatment for Mammary Tumors in Dogs & Cats
Nicole Ehrhart, VMD, MS, Colorado State University
Mammary Tumors in Dogs
In dogs, ≈50% of mammary tumors are benign; however, dogs with a history of benign mammary tumors are at increased risk for subsequent malignant tumor development, requiring ongoing monitoring and staging.
Up to 50% of malignant tumors metastasize, most commonly to regional lymph nodes and lungs. All dogs with suspected or confirmed mammary tumors should therefore undergo comprehensive staging, including physical examination, CBC, serum chemistry profile, urinalysis, 3-view thoracic radiography or thoracic computed tomography, abdominal ultrasonography, fine-needle aspiration of enlarged peripheral lymph nodes, and cytology to differentiate other tumor types (eg, mast cell tumors), although cytology cannot reliably determine benign versus malignant mammary tumors. Many tumor types have unique staging schemes devised by the World Health Organization (WHO; see Suggested Reading).
Surgical Technique
In dogs, mammary tumors should be excised using the simplest technique that allows complete removal with clean margins. Surgical approaches include:
Lumpectomy for small (<5 mm), well-encapsulated, mobile masses
Mammectomy for a single tumor affecting 1 gland centrally
Regional mastectomy for tumors spanning adjacent glands
Unilateral mastectomy for multiple tumors along 1 chain
Bilateral mastectomy or staged unilateral mastectomy for diffuse bilateral disease
Radical mastectomy for tumors fixed to underlying tissues or involving extensive local invasion
Pet owner education is essential. Additional masses are frequently identified after the patient is anesthetized and clipped. Informed consent should include authorization for expanding the planned procedure if additional tumors are found intraoperatively.
Surgical closure should be performed in 2 to 3 layers (ie, deep subcutaneous, superficial subcutaneous, skin).
Mammary Tumors in Cats
In cats, >80% of mammary tumors are malignant, a high percentage of which metastasize. Comprehensive staging, including physical examination, CBC, serum chemistry profile, urinalysis, 3-view thoracic radiography or thoracic computed tomography, abdominal ultrasonography, fine-needle aspiration of enlarged peripheral lymph nodes, and cytology, are imperative for understanding the extent of disease and future prognosis . Early and aggressive surgery is recommended because of the aggressive biological behavior of these tumors.
Surgical Technique
Early and aggressive surgery is recommended because of the aggressive biological behavior of these tumors. Best practice recommendations for cats with mammary tumors include total mastectomy, ideally performed as a staged bilateral procedure, in which stage 1 is unilateral mastectomy and stage 2 is contralateral mastectomy performed 2 to 4 weeks later. Radical mastectomy (taking additional fascial or muscle planes) is recommended if mammary tumors are attached to the body wall (uncommon).
Staging surgery minimizes wound tension, reduces postoperative complications, and allows the skin to stretch between procedures. Bilateral mastectomy in a single stage is not recommended due to excessive pain, impaired healing, and risk of respiratory compromise. Similar to dogs, closure should be performed in 2 to 3 layers.
All resected tissue should be submitted for histopathologic evaluation. Multiple tumors should be placed in separate containers and clearly labeled by gland location. Benign and malignant tumors commonly coexist in the same mammary chain.
Pain Management
Mastectomy procedures are associated with moderate to severe postoperative pain in both dogs and cats. Proper perioperative pain management is critical for animal welfare and because uncontrolled pain may impair immune function and promote tumor dissemination.
Recent research supports a multimodal analgesic approach, combining systemic medications with local/regional techniques.1
Key strategies include systemic analgesics, local anesthetic techniques, and regional anesthesia.
Systemic Analgesics
Opioids like methadone provide superior analgesia versus tramadol, particularly when administered preoperatively or intraoperatively.
NSAIDs reduce pain and inflammation and lower opioid requirements when administered in conjunction with gabapentin.
Ketamine CRI enhances opioid analgesia and may improve feeding behavior postoperatively.
Adjuncts like maropitant can be used for antinausea and anti-inflammatory effects; dexmedetomidine is an alpha-2 agonist that can provide analgesic effects.
Local Anesthetic Techniques
Infiltration Analgesia
Lidocaine or bupivacaine can be injected directly along the incision line. Needle-free devices or wound soaker catheters allow ongoing postoperative infusions. Safe systemic dosage limits for cats should not be exceeded.
Bupivacaine Liposome Injectable Suspension
Bupivacaine liposome injectable suspension is a long-acting local anesthetic approved for incisional administration in dogs and cats that provides sustained analgesia for up to 72 hours and is especially valuable in extensive surgeries (eg, mastectomy). This suspension should be infiltrated along the entire surgical site before closure. Manufacturer guidelines should be consulted for dilution, syringe preparation, and technique guidance.
Is tumescent local anesthesia safe in cats, and is it a good choice for feline mastectomy patients? Learn about the benefits—and risks—associated with this novel technique in this article on Tumescent Local Anesthesia in Cats Undergoing Mastectomy.
Regional Anesthesia
Epidural analgesia is useful for inguinal and caudal abdominal tumors. Morphine with local anesthetics provides lasting effect. Paravertebral block or transversus abdominus plane (TAP) block offers regional blockade of thoracic and abdominal walls, especially when combined with serratus plane blocks.Intercostal nerve blocks may be helpful when thoracic mammary glands are involved.
Take-Home Messages
Multimodal analgesia should be standard for all mastectomy patients.
Consideration should be given to combining NSAIDs, long-acting local anesthetics, and systemic opioids tailored to the species.
Regional blocks should be used for longer or more invasive surgeries.
Owner education regarding postoperative pain signs and medication administration is important.
All resected tissue should be submitted for histopathology and be clearly labeled by location.
Lumpectomy
Lumpectomy is used to remove small, BB-pellet–sized (<5 mm in diameter), freely movable masses not located directly under a nipple. A small cuff of normal tissue around the mass should be removed to ensure all tumor cells are extracted.
Mammectomy
Mammectomy is the removal of a single mammary gland, including the nipple and skin overlying the gland (Figure 1), and is a good choice when the mammary mass is directly under the nipple or fixed to the overlying skin. Mammectomy should not be used for masses fixed to the underlying rectus fascia.

Mammary tissue is superficial to the ventral fascia of the rectus muscle and typically has a layer of fat directly under the glands. All tissue should be removed down to the rectus fascia to ensure removal of the mammary gland. The rectus fascia and muscle should not be removed.
Regional Mastectomy
Regional mastectomy is indicated when a mammary mass is located between 2 glands or multiple small tumors are present in a section of the mammary chain (Figure 2). This technique should not be used for masses fixed to the underlying rectus fascia.

The skin, mammary tissue, and underlying fat should be removed (Figure 3). The rectus fascia and muscle should not be removed.

As necessary, the superficial inguinal lymph node should be dissected and the sample submitted separately for histopathologic evaluation to further determine the disease stage.
Mastectomy
Unilateral mastectomy involves removal of all mammary tissue on one side of the midline (Figure 4). Mammary tissue extends from midline to the nipple line and is an equal distance lateral to the nipple line.

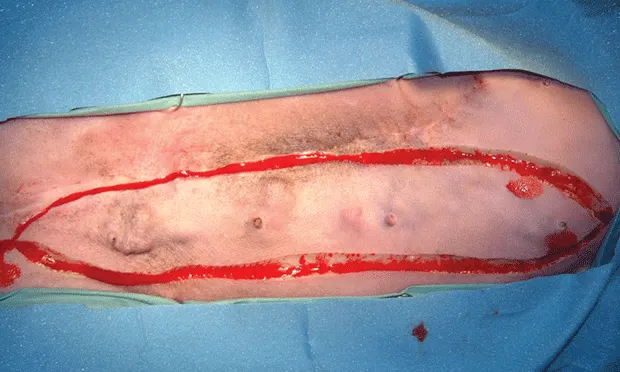
An elliptical incision should be made from the most cranial nipple to the most caudal nipple so that the medial extent of the ellipse is at midline and the lateral extent of the incision is equidistant on the lateral side of the nipple line (Figure 5).

All skin, mammary tissue, and fat down to the rectus fascia should be removed. The rectus fascia and underlying muscle should not be removed.
During caudal dissection, the caudal superficial epigastric artery and vein should be ligated to prevent excessive bleeding. These vessels run cranially under the mammary glands medial to the inguinal ring and anastomose with the cranial superficial epigastric vessels.
The superficial inguinal lymph node is typically contained within the fat underlying the inguinal mammary tissue. If possible, this node should be dissected and submitted separately for histologic evaluation to help further determine disease stage.
Unilateral mastectomy can be combined with lumpectomy on the opposite chain. If both mammary chains require mastectomy due to multiple masses, the side with the most disease should be removed first and the second mammary chain removed 2 to 4 weeks later for minimal complications related to skin tension.
Author Insight
Bilateral mastectomy performed as a single procedure often results in unacceptable skin tension and possible respiratory compromise (especially in cats) and has a high complication rate. Staged unilateral mastectomy is recommended when disease extent requires removal of both mammary chains.
Radical Mastectomy
Radical mastectomy involves removal of the mammary tissue and underlying rectus fascia, muscle, or body wall (Figure 6). This procedure is recommended for mammary tumors that are fixed to the underlying body wall. The plane of resection should involve 1 full tissue layer beyond the layer to which the tumor is fixed. For example, if the tumor is fixed to the rectus fascia, a layer of muscle deep to the area of fixation should be removed. In general, removal of fascia or partial-thickness body wall does not require body wall reconstruction. If full-thickness body wall resection is required, reconstruction methods should be followed to prevent herniation of abdominal contents.
In cats, mammary tissue extends to the skin overlying the caudal thorax. Avoiding penetration of the thoracic cavity is difficult in cats when partial-thickness body wall resection is attempted during radical mastectomy of the cranial mammary glands. Ventilation may be needed during anesthesia in case of inadvertent penetration of the thoracic cavity.


FIGURE 6