Intervertebral Disk Herniation
Intervertebral disk herniation (IVDH) is abnormal displacement of the nucleus pulposus and/or annulus fibrosus into the vertebral canal or intervertebral foramen. IVDH is the most common cause of spinal cord injury in dogs; some breeds have a lifetime incidence that approaches 20%.1
Noncontrast radiography of the vertebral column is often initially performed in suspected IVDH cases because images can be acquired rapidly and have high sensitivity and specificity for detecting certain diseases that can mimic IVDH (eg, diskospondylitis, vertebral column fracture/luxation). However, radiography is not a definitive means of identifying canine IVDH, as its accuracy is only 50% to 60% in the thoracolumbar vertebral column and 35% in the cervical vertebral column.2,3 Myelography, computed tomography (CT), and magnetic resonance imaging (MRI) are typically used to diagnose IVDH.
All three imaging modalities can localize spinal cord compression. Many clinicians favor MRI because it is multiplanar and noninvasive, provides data associated with functional outcome, and is the only means of diagnosing certain vertebral column diseases that clinically resemble IVDH (eg, vascular myelopathies).
Related Article: Methicillin-Resistant Staphylococcal Infections
Figure 1 (below). Lateral radiographs (A, C, and E) with corresponding T2-weighted sagittal MRIs (B, D, and F) obtained from 3 dogs with suspected IVDH based on clinical signs or survey radiographs; however, other causes were associated with spinal cord injuries in these clinical cases.(View larger image)
(A) Radiograph of the L3–4 vertebral articulation confirming severe disk space narrowing; reduction in the size of the intervertebral foramen; and smooth, bridging, ventral new bone formation.(B) Subsequent MRI identified increased T2 signal or a bright appearance within the central portion of the L3–4 disk space (*) and

ventrally located, extradural, T2 hyperintense (ie, bright) compressive material overlying the body of L4 (arrowhead). Surgical decompression, biopsy, and culture identified diskospondylitis and epidural empyema attributed to multidrug-resistant Staphylococcus aureus.

In a separate case, (C) cervical radiographs suggested disk space narrowing at C5–6 and C6–7, and (D) subsequent MRI showed centrally located spinal cord hyperintensity overlying the C5–6 vertebral articulation.This lesion was confirmed on necropsy as a spinal cord infarction caused by a fibrocartilaginous embolism.

In this dog, (E) vertebral column radiographs were within normal limits, but (F) a dorsally located dilation of the subarachnoid space (arrowheads) overlying the T13–L2 vertebrae with associated spinal cord compression was evident on the MRI.
Related Article: Vertebral Magnetic Resonance Imaging
Figure 2 (below).Lateral radiograph and myelogram showing classic features of canine IVDH. (View larger image)
(A) Lateral radiograph showing disk space collapse, disk space wedging, and reduced size and increased opacity of the intervertebral foramen at the T12–13 vertebral articulation. (B) Myelogram showing loss of the dorsal subarachnoid contrast column and dorsal elevation of the ventral contrast column over the T12–13 vertebral articulation.

These features suggest focal ventral extradural compression anatomically associated with the dorsal portion of the disk space. Although other diseases (eg, nerve sheath neoplasia) can result in this myelographic pattern, these features are relatively specific for IVDH.
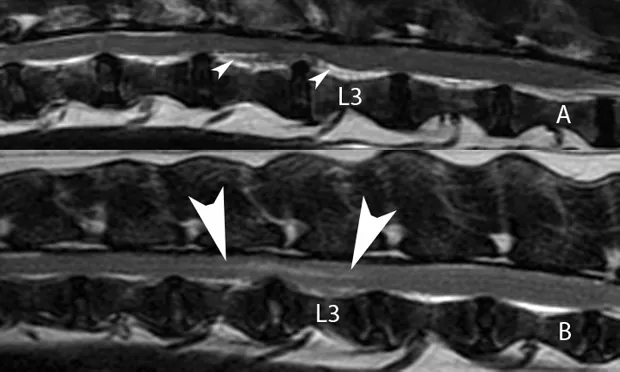
Figure 3 (below). Sagittal T2-weighted MRIs and sagittal bone window reconstructed CT image from three dogs with IVDH.(View larger image)
(A) MRI showing dispersed ventral disk extrusion at L2–3 (arrowheads) compressing the spinal cord without disturbing its signal (signal intensity color remains normal). (B) In this MRI, the dog has focal, nondispersed ventral disk extrusion subtly compressing the spinal cord

overlying the L2–3 vertebral articulation (arrowheads). The compressed spinal cord has central hyperintensity (arrowheads), which may indicate the presence of edema, necrosis, or hemorrhage and suggests adverse functional outcome. (C)

CT showing mineral dense or extruded disk material severely compressing the spinal cord at the T12–13 vertebral articulation (*). Although CT provides excellent distinction between mineralized disk material and soft tissues, soft tissue contrast is inferior to that on MRI.
Figure 4 (below). Transverse T2-weighted MRI and soft tissue windowed CT images confirming IVDH in two dogs.(View larger image)
(A) MRI clearly showing ventrally located extruded disk material (*) that is hyperintense relative to the dorsally located, compressed spinal cord. Extruded disk material may appear hyperintense on T2-weighted images when inflammatory infiltrates, hemorrhage, or nonmineralized nuclear materials are present. (B) CT image showing left-sided ventrolateral, extradural compression associated with disk extrusion (arrowhead). Density of the compressing material is consistent with hemorrhage, which can be a significant source of

compression if disk material lacerates the ventral vertebral sinuses.