
Projectile injuries (eg, gunshot wounds, arrow wounds) are rare in veterinary medicine. Ballistic injury accounts for 1% of trauma cases in both dogs and cats, and impalement has a 5.4% prevalence in dogs and a 3% prevalence in cats.1
Although uncommon, cases involving projectile injuries can require high acuity, result in increased levels of stress, and be emotionally taxing for the veterinary team. Preparation, competence, communication, and leadership are critical.
This article describes a dog with a gunshot wound and uses the framework of the Veterinary Advanced Trauma Life Support (VetATLS) course to demonstrate key aspects of assessment, management, communication, and teamwork (Figure 1).
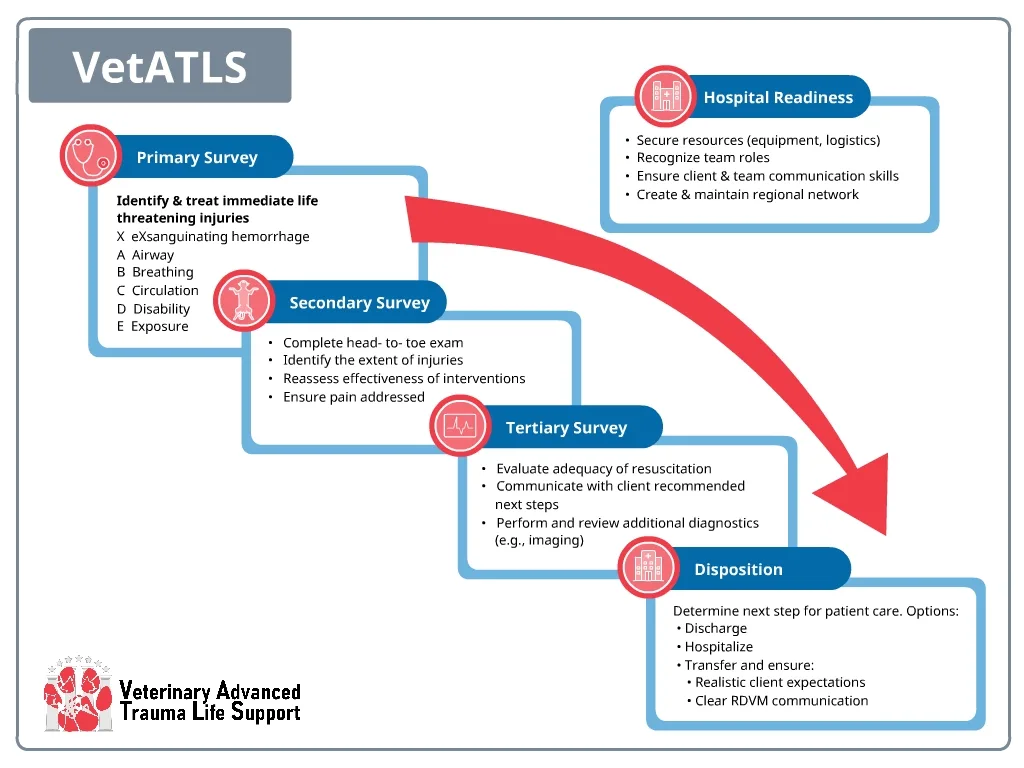
FIGURE 1 Process map for triage and care of veterinary trauma patients from intake through disposition. RDVM, referral veterinarian. Image used with permission from the Veterinary Committee on Trauma, the American College of Veterinary Emergency and Critical Care, and Colorado State University; all rights reserved.
Some of the content and visual aids in this article are from the VetATLS course, which is designed for clinicians and veterinary team members who want to enhance their confidence and competence in managing patients with emergent trauma.10
Case Presentation
Ricky, an 8-year-old spayed Australian shepherd dog, was presented for difficulty breathing (ie, shallow, quick) of 1-hour duration after being loose in a field behind the owner’s house. The owner noted that Ricky is not aggressive and is known to enjoy exploring.
Initial Assessment & Management
Primary Survey
Patients with traumatic injuries should undergo a primary survey as soon as they are presented to the clinic to allow quick identification of injuries and provision of interventions in order of priority (Figure 2).2 In cases of projectile injury, the extent of damage may be hidden, and pet owners might not realize the dog has sustained a penetrating injury.

FIGURE 2 Primary survey chart outlining steps for evaluation, critical findings, tools, adjuncts, and interventions for each major step. aBG, arterial blood gas; CRT, capillary refill time; MGCS, modified Glasgow Coma Scale; PCV, packed cell volume; TP, total protein; T-POCUS, thoracic point-of-care ultrasound.Image used with permission from the Veterinary Committee on Trauma, the American College of Veterinary Emergency and Critical Care, and Colorado State University; all rights reserved.
The XABCDE Framework
X – Exsanguination: Control massive external hemorrhage first. A blood sweep, in which all sides of the patient are inspected visually and with a tactile sweep through the fur to look for significant blood, is recommended to look for hemorrhage.
A – Airway: Determine whether the airway is patent.
B – Breathing: Evaluate respiratory effort and adequacy.
C – Circulation: Assess perfusion and hemodynamic status.
D – Disability: Perform a brief neurologic examination.
E – Exposure/Environment: Visually examine the entire body; look for wounds, burns, or other traumatic injuries that could result in rapid thermal or fluid loss.
Initial Interventions Based on the Primary Survey
After the primary survey is complete, pain medications can be administered. Full mu-opioid receptor agonists (eg, methadone, morphine, hydromorphone) are recommended.
Many potential causes of an abnormal breathing pattern are possible in patients with sustained trauma, including pneumothorax, pulmonary contusions, hemothorax, rib fractures, diaphragmatic hernia, pain, and shock.
Thoracic auscultation is typically the first step in narrowing the list of differentials. If available, thoracic point-of-care ultrasound (POCUS) may help determine the cause of the abnormal breathing. If POCUS is unavailable, radiography should be performed following the primary survey and initial stabilization.
An IV catheter may be placed and a small fluid bolus of isotonic crystalloids (10-20 mL/kg) administered if indicated.3 Perfusion parameters (eg, mentation, heart rate, pulse quality, mucous membrane color, capillary refill time) should be assessed before and after the fluid bolus is given to determine the effect of the intervention and whether additional fluids are needed.
What If Something Is Stuck?
If a foreign object (eg, an arrow, a piece of rebar, shrapnel) is embedded in the patient’s body, the material should not be immediately removed. Premature removal can result in hemorrhage or pneumothorax. Removal can be initiated after the patient has been stabilized, a secondary survey (ie, full physical examination, patient history) has been performed to identify all traumatic injuries, and vascular access has been obtained. Ideally, removal should occur with the patient under general anesthesia, and a plan for definitive surgical care should be in place.
If the object can be cut without excessive manipulation, the protruding surface may be shortened to minimize the potential for internal damage through inadvertent jostling. If the patient must be transported to another facility or a significant delay is expected before surgery, a protective bandage should be placed around the penetrating object to help stabilize the object and to prevent air from entering the wound, which could cause an ongoing pneumothorax.
What If a Pneumothorax Is Found on Thoracic POCUS or There Is Concern for Pneumothorax?
Thoracic POCUS can be used to evaluate for a pneumothorax by looking for the absence of lung sliding (ie, no glide sign).4 In cases in which the glide sign is absent, the pleural line appears static, indicating the visceral pleura is no longer contacting the parietal pleura due to air filling the space. Thoracic POCUS can also help diagnose pulmonary contusions (a differential in trauma patients that requires oxygen therapy) via presence of B-lines.5
If a pneumothorax is diagnosed and the patient is experiencing respiratory difficulty, thoracocentesis should be performed.6 If a second thoracocentesis is necessary because of the continued build-up of air, then placement of a chest tube is indicated.7
Ricky’s Primary Survey Results
Ricky’s respirations appeared short and shallow, suggestive of either pulmonary contusions or pneumothorax (Table 1). Thoracic POCUS showed loss of the glide sign, increasing concern for a pneumothorax. Thoracocentesis was performed, and 800 mL of air was removed from the right side of the chest.
Secondary Survey
The secondary survey includes performing a full physical examination, reassessing all vital signs, and obtaining pertinent diagnostics to identify the extent of injuries and determine the next diagnostic and treatment steps (Figure 3). The secondary survey does not begin until the primary survey is complete, resuscitative efforts are underway, and vital parameters have improved. If the patient’s status changes at any point during the secondary survey, the primary survey should be reinitiated. A goal of the secondary survey is to visualize all wounds and make a plan for imaging and definitive wound care.

FIGURE 3 The secondary survey chart outlining critical findings, tools, adjuncts, and interventions. CT, computed tomography. Image used with permission from the Veterinary Committee on Trauma, the American College of Veterinary Emergency and Critical Care, and Colorado State University; all rights reserved.
Ricky’s Secondary Survey Results
Ricky’s secondary survey results (Table 2) show penetrating wounds to the thorax.
What Should Be Communicated to Pet Owners at This Point?
After the primary survey is complete, initial stabilization has been performed, and the secondary survey is complete, the owner should be educated on what has been found so far, what interventions have been performed, what the immediate concerns are, and what the next steps should be.
Prognosis should not be determined unless the condition is clearly grave or clearly stable. Honesty regarding unknown elements should be communicated while reassurance is still provided to the owner. Potential financial costs of further care, whether a referral is likely, and/or decisions about continued diagnostics or interventions should be discussed at this time.
Tertiary Survey
A tertiary survey allows re-evaluation for any delayed or missed injuries and should include additional diagnostics approved by the owner, documentation, management, and referral (if indicated) for all noted injuries. The tertiary survey should begin as soon as possible after the primary and secondary surveys and should be completed no later than 24 hours after initial presentation.
Interventions at this stage may include clipping, cleaning, and covering of the wound. For projectile wounds, the entry and exit wounds (if present) should be covered. When the wounds are clipped and cleaned, the patient should be under sedation and closely monitored, as disruption of blood clots or other tissue can suddenly worsen the pneumothorax and cause the patient to become unstable quickly.
Non-POCUS imaging of the thorax may also be considered. In most cases of projectile injury, radiography of the injured area may be sufficient, especially if the primary clinical question is whether the projectile or fragments of the projectile remain in a limb or cavity; however, whole-body CT (ie, trauma CT) may be more appropriate if damage seems extensive, multiple projectiles are present, patient stability is declining, or surgery is imminent without a clear plan. Trauma CT, if available, can offer a sensitive and specific modality for recognition of injuries sustained by a patient with polytrauma.8 Although CT is likely more expensive than repeated radiography, CT often provides results more quickly. CT can often be performed with the patient under heavy sedation that is appropriate for a trauma patient and careful monitoring during the scan. Trauma CT is thus considered a first-choice imaging modality for critical polytrauma patients.
Ricky’s Tertiary Survey Results
Radiographs showed multiple small, metallic foreign bodies in the chest and abdomen consistent with BB Shot (Figure 4). Continued presence of pneumothorax was also observed. The owner should be informed that the mechanism of injury is clear. Ricky will need more aggressive supportive care because he did not stabilize after the first thoracocentesis. Because thoracocentesis has already been performed, placement of a thoracostomy tube is indicated, and continuous suction may be considered if air continues to build up between hand aspirations. Approval for a thoracostomy tube should be discussed with the owner.


FIGURE 4 Lateral (left) and ventral (right) radiographs showing the presence of metallic foreign bodies and evidence of pneumothorax (arrows).
Disposition
Disposition options include obtaining additional diagnostics, proceeding to surgery, admitting the patient to the hospital, discharging the patient home, or pursuing humane euthanasia.
Surgery is indicated for most projectile injuries because of the ability to remove foreign material, the need for hemorrhage control, and the benefit of debridement and lavage. Dogs with projectile injuries may be managed similarly to dogs with blunt thoracic trauma if no major abnormalities are found on imaging and the patient is stable.
Ricky’s Disposition Results
Based on Ricky’s radiographs, surgery to remove ballistic particles and evaluate lungs for potential rupture should be recommended. The pneumothorax could be air coming in from the environment from the disruption in the chest wall or from a ruptured lung.
With thoracotomy, prognosis is suspected to be good. Thoracotomy for penetrating trauma is debated among veterinary surgeons, and the advantages and disadvantages for each patient should be clearly outlined. In some cases, hospitalization until the pneumothorax resolves can be a good option. See below for discussion if surgery is not pursued.
Client Communications & Finances
Financial Limitations
Financial limitations are a common factor in projectile injury cases because the condition can be severe and not anticipated. If the patient remains unstable after intervention and attempts at resuscitation, and financial limitations are a concern, humane euthanasia should be discussed with the owner. If the patient is stable, a plan involving conservative management with monitoring and pain medications can be pursued. Owners should be warned that dogs with traumatic injuries can decompensate quickly, especially in the first 24 hours after injury.
Emotional Support
Cases involving projectile injuries can be emotionally difficult. Communications should be clear, compassionate, and frequent. Owners may experience a range of emotions, including shock, guilt, anger, or fear, especially if the injury was intentional or involved a firearm. Veterinary teams should approach these situations with empathy and without judgment.
Taking time to actively listen to the owner’s concerns is important; care on what is stated to the owner is advised (see Potential Legal Issues). Simple, nontechnical language should be used when discussing prognosis, diagnostics, and treatment options, and breaks should be taken frequently to check for understanding and emotional reactions.
Potential Legal Issues
There are important guidelines to consider if there is possibility for a criminal case or civil suit.9
Document everything: Injuries should be photographed and added to the record if possible.
Do not speculate: Neutral language that does not imply guilt should be used.
Know your state’s reporting obligations: In most states in the United States, suspected animal abuse is mandated to report.
Prioritize patient safety: If the patient is being returned to a potentially unsafe situation, options can be discussed with local law enforcement or animal control. Direct intervention without support should not be attempted.
Potential for Future Injuries
In cases involving projectile injury, the injury may have been intentional, and the patient may remain at risk for further injury. This issue should be approached delicately with the owner. Concern for the patient’s safety should be balanced with sensitivity toward the owner (see How to Ask Delicate Questions). These conversations should be documented clearly in the record.
How to Ask Delicate Questions
“I need to ask a couple of difficult but important questions due to the nature of the dog’s injury.” (pause)
“Do you have any reason to believe this injury may have been intentional?” (give space for a response)
“Is there any chance there may be other injuries that we haven’t found yet, either from this incident or anything else that concerns you?”(give space for a response)
“Do you feel safe? Would it help to connect with local animal control or law enforcement?”
Conclusion
Projectile injuries in dogs are rare but require rapid assessment, structured management, and compassionate communication. By using a systematic approach, veterinary teams can prioritize handling life-threatening issues, stabilizing patients, and making informed decisions about imaging, surgery, and ongoing care.
Beyond the medical aspects, these cases demand emotional support for both pet owners and veterinary staff, as well as careful documentation and awareness of potential legal implications. Preparation, empathy, and teamwork are essential for delivering high-quality, ethical care in these high-stakes situations.