Fluid Therapy: The Critical Balance Between Life and Death
Intravenous fluid therapy is essential for treatment of a variety of acute and chronic critical illnesses. Without careful observation and monitoring, however, intravenous fluids can contribute to a patient's morbidity and, potentially, mortality. A careful understanding of a fluid's indications and contraindications is required when making fluid choices in a critically ill animal, particularly those with cardiac disease, hypoalbuminemia, metabolic disturbances, coagulopathies, or systemic inflammation.
Related Article: Synthetic Colloid Fluids & Volume Expansion
Fluid Overload
Intravenous fluids can be subdivided into two broad categories: crystalloids and colloids. Crystalloid fluids contain ionic particles in solution. The components of each fluid type can be used to treat specific metabolic and electrolyte abnormalities in addition to correcting intravascular and interstitial fluid and electrolyte deficits. Overzealous use of crystalloids can promote leakage of fluid into the interstitial fluid compartments as well as the pulmonary alveolar space, resulting in interstitial and pulmonary edema.1,2 These problems can be compounded by promotion of intravascular volume overload and can cause pulmonary edema in patients with cardiovascular disease.
Colloid fluids contain large particles in solution that attract water around their core structure. Once a colloid is infused into the bloodstream, the colloid particles aid in retaining water or fluid within the intravascular space.1,2 The Gibbs-Donnan effect pulls water into the intravascular space and holds it around the core structure of the colloid particle within the blood vessel.
The Starling equationV = [kf(Pc - Pif) - σ(πc - πif)] - Qlymph
describes the relationship of the forces that retain fluid within the intravascular and interstitial fluid compartments of the body.1,2 V is the net flow of fluid, kf is the filtration coefficient, Pc and Pif are the hydrostatic pressure within the capillary and interstitial fluid spaces, σ is the pore size within the capillary membrane, πc and πif are the colloid oncotic pressure within the capillary and interstitial fluid spaces, and Qlymph is the rate of lymphatic drainage of fluid from the interstitium.3 The force with which a crystalloid pushes fluid out of a compartment is known as hydrostatic pressure. The force of a colloid that retains fluid within a compartment is known as the colloid oncotic pressure.1,2 Other factors, including vascular permeability and the ability of the lymphatic system to drain fluid, are involved in fluid retention or leakage from vessels into the interstitial matrix.1,2
Related Article: Shock Fluid Therapy in Cats
Under normal circumstances, the hydrostatic pressure within the pulmonary capillary beds is approximately 10 mm Hg.4 The oncotic pressure within the pulmonary interstitium is roughly 25 mm Hg-the net effect favors retention of fluid within the interstitial space. If aggressive administration of intravenous crystalloid or colloid fluids causes a rapid increase in pulmonary vascular hydrostatic pressure that exceeds 25 mm Hg, fluid leaks into the interstitial matrix and overwhelms the pulmonary lymphatic drainage system. This is particularly important in animals with mitral valvular insufficiency or decreased myocardial contractility.4
Predisposing Factors
InflammationConditions that cause severe inflammation can also disrupt the tight junctions of the endothelium within the pulmonary vasculature and cause interstitial and alveolar fluid accumulation after administration of a relatively small volume of intravenous fluid. Because of increased capillary pore size in inflammation, fluid can leak into the interstitium, causing alveolar flooding even in the absence of elevated pulmonary capillary hydrostatic pressure.5
AlbuminAlbumin contributes approximately 80% to the colloid oncotic pressure of blood. Severe hypoalbuminemia (< 2.0 g/dl) can allow peripheral and pulmonary edema fluid accumulation, due to decreased interstitial albumin concentration.3 Clinical conditions that may be associated with severe hypoalbuminemia include ascites, protein-losing enteropathy or nephropathy, burns and other exudative wounds, and end-stage hepatic disease.3 Administration of large volumes of crystalloid fluids alone, without addition of natural or synthetic colloids, may exacerbate subcutaneous or pulmonary edema in hypoalbuminemic patients.1-3 Thus, natural or synthetic colloids should be used in conjunction with crystalloid fluids to avoid these complications.
Hetastarch is a large-molecular-weight polymer of amylopectin (Abbott Laboratories), is widely available, and is a cost-effective synthetic colloid for use in general practice. Hetastarch is broken down by serum amylase and can bind with von Willebrand's factor. In animals that have received hetastarch, serum amylase may be elevated. Activated partial thromboplastin time or activated clotting time may be slightly prolonged but is clinically irrelevant after its use.
Related Article: Placement of Central Venous Catheters
Prevention of Iatrogenic Fluid Overload
The CVP is a measure of hydrostatic pressure in the anterior vena cava.6 Although not a direct measure of the pressure downstream in the pulmonary capillary matrix, CVP is used as an indicator of vascular volume and can be used to help gauge intravenous fluid therapy volume requirements in patients susceptible to vascular volume overload.6,7 Susceptible patients include those with cardiovascular disease, renal insufficiency or failure, systemic inflammation, or hypoalbuminemia.3
The patient's CVP (in cm H2O) is the lowest point of the meniscus when the fluid column stops moving. Repeat the measurement several times and calculate the average pressure to enhance the precision of measurement. To facilitate accurate comparisons, always place the animal in the same position (eg, lateral or sternal recumbency) when taking subsequent measurements. Normal CVP for dogs and cats is less than 5 cm H2O. As a general rule, to avoid volume overload a patient's CVP should not increase more than 5 cm H2O within a 24-hour period.1
In hypoalbuminemic animals, colloid oncotic pressure can be measured with a colloid osmometer.8 Normal colloid oncotic pressure values are 19.95 ± 2.1 mm Hg for dogs and 24.7 ± 3.7 mm Hg for cats.9 In many veterinary hospitals, however, measurement of colloid oncotic pressure is impractical because of the lack of necessary equipment. Normally, serum albumin values comprise approximately half of a patient's total protein values in the circulation3 and knowledge of a patient's serum albumin and globulin concentrations is sometimes helpful as a rough indicator of whether colloid support is necessary. If total serum protein is less than 4.0 g/dl or serum albumin is less than 2.0 g/dl, administration of such colloids as hetastarch (20 to 30 ml/kg per day), fresh frozen plasma (20 ml/kg), or concentrated 25% human albumin (2 ml/kg)10 should be considered.
If colloids are administered concurrently with crystalloids, decrease the crystalloid volume by 25% to 50%.1 An intravenous fluid pump or in-line flow regulator avoids iatrogenic fluid overload due to inadvertent opening of the clamp on the intravenous fluid line. This is especially important in small patients.
What You Need to Measure Central Venous Pressure
Manometer or length of IV extension tubing attached to a metric ruler
Sterile 0.9% saline
20-ml syringe
Three-way stopcock
How to Measure Central Venous Pressure
Place a central venous catheter in the jugular vein such that the distal tip of the catheter is seated just outside of the right atrium.

Confirm catheter placement with a lateral thoracic radiograph (Figure 1. Lateral thoracic radiograph of jugular central venous catheter. Note that thedistal catheter tip (arrow) is located just outside of the right atrium).* Attach the 20-ml syringe directly to the female port of the 3-way stopcock.
Connect the manometer (or other length of IV extension tubing attached to a metric ruler) to the other female port of the stopcock.
Attach the male port of the stopcock to the female end of the IV extension tubing, which is attached to the jugular catheter.
Place the patient in lateral or sternal recumbency, and turn the stopcock off to the patient. Infuse saline (0.9%) into the manometer-take care not to introduce air bubbles into the apparatus.

Hold the 0-cm marker on the manometer at the patient's sternum/manubrium, or at the point of the elbow (Figure 2. Patient in lateral recumbency to measure central venous pressure from a central venous catheter placed in the jugular vein. The 0 point on the ruler is adjusted so it is adjacent to the point of the elbow).
Turn the stopcock on to the patient and off to the syringe to allow the fluid column to drop and equilibrate with the patient's intravascular volume.
Fluid RequirementsMetabolic fluid requirements are roughly equivalent to metabolic energy requirements. Since it takes 1 ml of water to metabolize 1 kcal of energy, metabolic fluid requirements can be calculated by the following formula: (30 × body weight in kg) + 70 = ml water required/d.11,12
In many critically ill animals, the patient's daily requirements are significantly increased by the need for fluid diuresis and replenishment of intravascular and interstitial volume deficit because of ongoing losses due to vomiting, diarrhea, and wound exudates.1-3 As a rule, the patient's dehydration deficit should be clinically estimated; then fluid requirements should be calculated, aiming to replenish 80% to 100% of the deficit in addition to maintenance requirements over a 24-hour period.1,2 Acute losses of body weight in critically ill animals are largely due to fluid losses.1,2 Because 1 ml of fluid roughly weighs 1 gram, fluid losses can be measured by monitoring body weight regularly and accurately, thereby enabling safe replenishment of fluid deficits, rather than using "guesstimates" and potentially causing iatrogenic volume overload.
Treatment of ComplicationsClinical signs of overhydration include tachypnea, orthopnea, serous nasal discharge, chemosis, pulmonary crackles, and subcutaneous pitting edema (Figures 3 and 4). In animals with renal insufficiency or failure, careful titration of fluid therapy is essential, as decreased urine output may result in intravascular volume overload.

Figure 3. Chemosis in a dog with intravascular and interstitial fluid volume overload. This patient had oliguric renal failure.

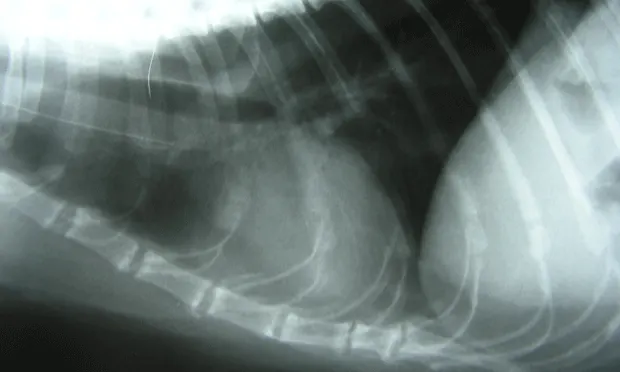
Figure 4. Lateral thoracic radiograph of a patient with pulmonary edema secondary to fluid overload.
If clinical signs of overhydration develop, intravenous fluids should be discontinued, and 2 mg/kg IV furosemide administered to promote diuresis. Conditions that can predispose an animal to overhydration, such as renal failure, cardiac disease, systemic inflammation, and hypoproteinemia, should be investigated on a case-by-case basis.
Related Articles:Poor Perfusion: Stabilization & Fluid ResuscitationShock Fluid Therapy in Cats