Dyspnea in a Cat
Mark Rishniw, BVSc, MS, PhD, DACVIM (Internal Medicine & Cardiology), Cornell University

A 6-year-old Persian is presented for acute dyspnea.
History
A heart murmur was detected on auscultation 1 year previously during a routine examination but was not pursued diagnostically at the time. Heartworm prophylaxis has been given consistently. The owners report that the cat has been slightly quiet over the past 3 days and has had a decreased appetite. This afternoon, the cat was distressed and dyspneic.
Physical Examination
A soft systolic parasternal murmur and gallop sound are noted onauscultation. The cat is tachycardic (heart rate, 240 beats/min) and severely dyspneic (respiratory rate, 90 breaths/min; open-mouth breathing). Mucous membranes are pale pink. Lung sounds are not easily detected on auscultation. Femoral pulses are palpable.
Ask Yourself . . .
Based on the historical and clinical findings, what is the best course of action?
Obtain thoracic radiographs and echocardiography.
Perform pleurocentesis and administer oxygen and diuretic therapy.
Perform anesthesia and bronchoscopic examination.
Administer antibiotics, bronchodilators, and glucocorticoids.
Correct Answer: Perform pleurocentesis and administer oxygen and diuretic therapy.
The history and clinical findings primarily suggest CHF or other causes of pleural effusion. Less likely are feline asthma, lungworm, heartworm, or pneumonia. The reduced intensity of lung sounds suggests pleural effusion. There is no history of coughing, which is usually present with primary pulmonary diseases, but commonly absent in cats with CHF.
Cats with severe CHF are fragile. Excessive handling, restraint, and diagnostic testing can lead to dramatic clinical decompensation and even death. Pleurocentesis is relatively safe and often less stressful than radiography in diagnosing pleural effusion. If effusion is diagnosed, it can be drained in the same procedure, substantially alleviating the dyspnea.
How to Proceed
Pleurocentesis is performed bilaterally with a narrow-gauge butterfly needle (21 to 23 gauge) attached to a three-way stopcock and 10-ml syringe (Figures 1 and 2). Shave and aseptically prepare a small region of the ventral chest wall. Gently restrain the cat-do not sedate-while it is seated or in sternal recumbency. Carefully insert the needle between two ribs while gently aspirating the fluid. Once the syringe is filled, hold the needle in position while expelling the fluid from the syringe via the stopcock.
FIGURE 1 A butterfly needle with stopcock and syringe are used for diagnostic and therapeutic pleurocentesis.

FIGURE 2 Pleurocentesis is performed with gentle restraint.
After pleurocentesis, or if no fluid is found, administer furosemide IV, IM, or SC if peripheral catheter placement is likely to unduly stress the patient. Administer supplemental oxygen using an oxygen cage, as nasal oxygen catheters or face masks usually cause stress.
Handle the cat as little as possible during stabilization. Record respiratory rate and effort every 30 to 60 minutes. Administer furosemide every hour if IV and every 2 to 3 hours if IM or SC, until respiratory effort and rate are substantially improved. If there is no improvement after 4 to 6 hours, reexamine the presumptive diagnosis. Fluids should not be administered parenterally, but water should be available ad libitum.
Once the patient is stabilized (often after 12 to 24 H), obtain radiographs (Figure 3) and echocardiography to confirm the diagnosis of CHF and to identify the nature and severity of the cardiac disease. The most common cause of CHF in cats is HCM; less common are dilated, restrictive, and unclassified cardiomyopathy. Murmurs associated with HCM are usually created by mitral regurgitation, abnormal displacement of the mitral valve during systole (systolic anterior motion or SAM), causing left ventricular outflow tract obstruction, or dynamic right ventricular obstruction either in combination (e.g., mitral regurgitation is always present with SAM) or alone (mitral regurgitation can also occur without SAM) (Figure 4).
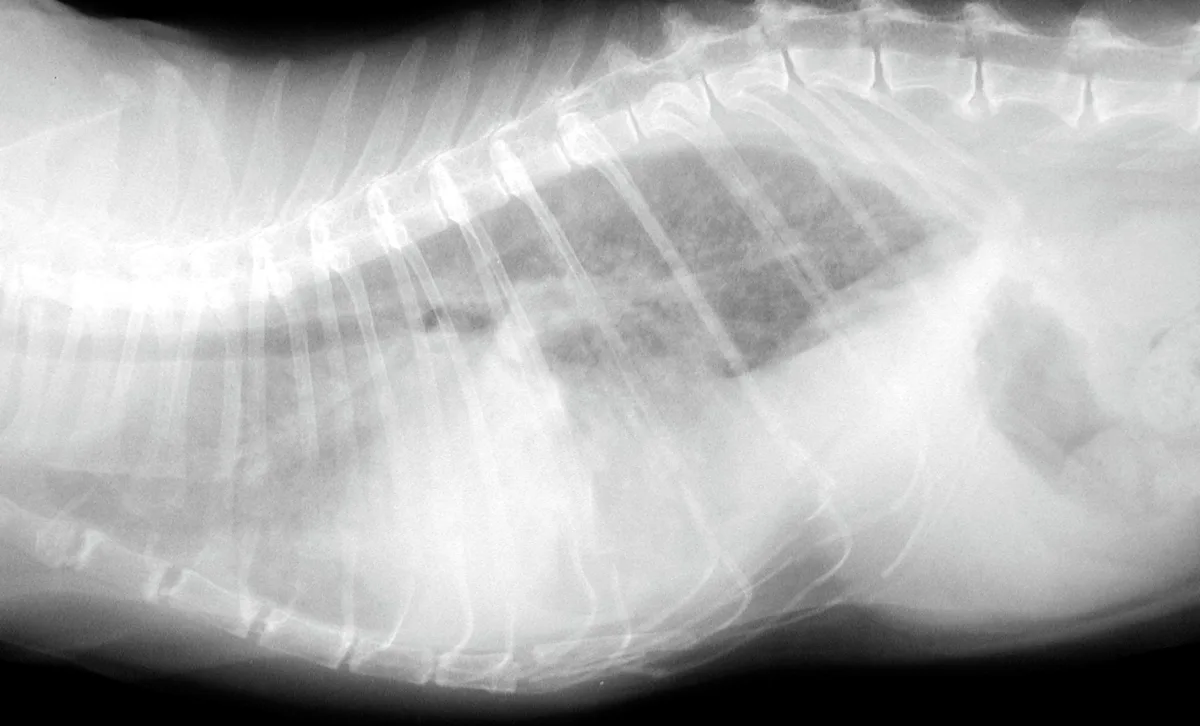
FIGURE 3 Lateral (A) and dorsoventral (B) radiograph of a cat with pleural effusion and suspected cardiomegaly; the radiograph was obtained after stabilization.

FIGURE 4A Two-dimensional, right parasternal, long-axis view of the heart in a cat with HCM and pleural effusion. Note the large thrombus in the left atrium
Ongoing Treatment
Cats with HCM and CHF generally require indefinite treatment with oral furosemide and ACE inhibitors upon discharge. Recent studies suggest that the calcium-channel blocker diltiazem and β-blockers do not alter survival in these patients-and may even decrease survival-so their use is controversial. Average survival of cats with HCM is 12 to 24 months once CHF occurs.
Take-Home Messages
Cats with CHF or other causes of pleural effusion are often dyspneic but do not typically cough.
Pleural effusion occurs with biventricular CHF in cats.
Stress can cause abrupt clinical deterioration: minimize stress in cats with severe dyspnea by avoiding excessive diagnostics and handling.
Confirm the diagnosis with radiographs and echocardiography only after the patient is stable enough to tolerate the procedures.
HCM is the most common acquired cardiac disease in cats.
Treatment at a Glance
To rapidly stabilize the patient, perform diagnostic and therapeutic pleurocentesis if pleural effusion is confirmed or strongly suspected.
Administer furosemide IV, IM, or SC until dyspnea improves substantially.
Treat long-term with ACE inhibitors and furosemide.
Use of diltiazem or β-blockers is controversial and is best reserved for those cases with dynamic outflow tract obstruction.