Treatment of Lumbosacral Disease
Stephanie Kube, DVM, DACVIM (Neurology), CVPP, CCRT, Veterinary Neurology and Pain Management Center of New England, Walpole, Massachusetts
Jacklyn T. Wolfe, DVM, Veterinary Neurology and Pain Management Center of New England, Walpole, Massachusetts

You have asked...
How do I treat lumbosacral disease?
The experts say...
Lumbosacral (LS) disease refers to any disease process that affects the L7-S1 junction. LS disease is also referred to as cauda equina syndrome (CES), a pathologic condition that affects the last pairs of spinal nerve roots, their related vasculature, or both.1-4
Lumbosacral disease is a multifactorial degenerative disease that primarily affects middle-aged-to-older large-breed dogs, with male dogs more commonly affected (2:1). German shepherd dogs are the most likely to develop this disease, but it has been reported in a variety of dog breeds, and it is increasingly recognized in cats.1,4,5
Lumbosacral Disease, AKA:
Lumbosacral syndrome
Lumbosacral stenosis
Degenerative lumbosacral stenosis
Lumbosacral instability
Lumbosacral malformation
Lumbosacral disease has both anatomic and degenerative factors. The most common cause is lumbosacral stenosis (narrowing of the vertebral canal) at the level of the lumbosacral joint. This narrowing can be caused by degenerative changes to the intervertebral disk or joint and scarring or abnormal proliferation of the surrounding ligaments; this can include the dorsal longitudinal ligament and the interarcuate ligament.1,3,4
Anatomically, dogs with abnormal shape to their last lumbar or sacral vertebrae and transitional vertebrae (eg, German shepherd dogs) are predisposed to lumbosacral stenosis.6-8 Other causes of lumbosacral disease include neoplasia, disk extrusion or protrusion, diskospondylitis, and trauma.1,3,4,6,9
Anatomic Review
Dogs have 7 cervical, 13 thoracic, 7 lumbar, 3 sacral, and a variable number of caudal vertebrae. The level at which the spinal cord terminates within the vertebral canal varies depending on the size of the dog. In large-breed dogs, the spinal cord tends to terminate more cranially than in small-breed dogs—the average being at the level of L6. The cauda equina, which is the bundle of spinal nerves and nerve roots remaining after the termination of the cord, contains spinal nerves +/-L5, L6, L7, S1-3, and Cd1-Cd5. Cauda equina syndrome is caused by involvement of 1 or more of these nerves.2
Related Article: Ambulatory Paraparesis in a German Shepherd Dog
History
The owner may report a variety of concerns. Affected patients may frequently display unilateral or bilateral pelvic limb lameness. The owner may report that the pet shows signs of: pain when touched near the pelvic region; self-mutilation; dragging or scuffing toes; reluctance to climb into the car or ascend stairs; low tail carriage; stiffness in the pelvic limbs; and/or difficulty rising or positioning to urinate or defecate. In severe cases of nerve root compression, the owner may report urinary and/or fecal incontinence. The owner may describe that these signs appear more evident after the patient has been working or playing.4,5
At a Glance: Cauda Equina Syndrome/Lumbosacral Stenosis
Large-breed dogs are often affected, especially German shepherd dogs
Most common cause of LS pain in dogs
Male:female ratio is 2:1
Average age of onset is 7 years
Common in working dogs
Clinical Findings
The examination should include a full neurologic and orthopedic examination. Any of the following may be observed:
Hyperesthesia of the LS region during palpation and tail hyperextension/manipulation.
The lordosis test is another way to assess the LS region.
The test involves the extension of the lumbosacral joint; pressure is placed on the LS region from a dorsal direction with the pelvis supported to avoid hip extension and confusion regarding coxofemoral osteoarthritis.
The authors do not routinely perform this test because it is thought to cause the patient undue pain.
Unilateral or bilateral lameness
Paraparesis
Muscle atrophy
Decreased withdrawal reflex
Decreased gastrocnemius reflex
Pseudohyperreflexia of the patellar reflex secondary to removal of the antagonistic impact of the caudal thigh muscle nerve supply
Changes in anal tone and a flaccid bladder may also be noted. At times, neurologic findings may be subtle.
Related Article: Orthopedic Examination of the Rearlimb in the Dog
Important Rule-outs
A thorough orthopedic examination is important in ruling out hip dysplasia and coxofemoral osteoarthritis; many of the clinical manifestations of these diseases closely mimic one another and often occur concurrently. Other differentials to consider include:
Metabolic disorders causing weakness
Myopathies
Myasthenia gravis
Cranial cruciate ligament injuries
Polyarthropathies
Iliopsoas muscle injury
Primary malignant neoplasms (eg, osteosarcoma, hemangiosarcoma, fibrosarcoma, nerve sheath tumors)
Metastatic (prostatic) neoplasia
Inflammatory disease
Fracture/luxation
Diagnostic Imaging
The gold standard for advanced imaging in the diagnosis of lumbosacral disease is MRI, but survey radiography should be performed before MRI.
Survey radiography of the lumbar spine, pelvis, and hips is recommended. Common abnormalities identified in patients with LS disease include vertebral spondylosis, sclerosis of the vertebral end plates, and collapsed L7-S1 disk space. Stress radiography may exacerbate a lumbosacral step, which can further aid in diagnosis. Radiographs are also recommended to help rule out metastatic disease, diskospondylitis, trauma, or luxation (Figures 1-3).
MRI is the diagnostic procedure of choice because it can identify soft tissue (eg, cauda equina, epidural fat, intervertebral disk) at the lumbosacral region without use of contrast (Figures 4 and 5).

Figure 1
Right lateral radiograph of a dog demonstrating L7 fracture. Images courtesy of Dr Tammy Stevenson.
Additional imaging (eg, diskography, epidurography) has been performed in the past and may be useful. Electrodiagnostics such as electromyography and nerve conduction studies may also be helpful.
Treatment
Medical and surgical management options are available. When discussing the options with the owner, it is important to keep in mind the desired outcome and owner expectations.
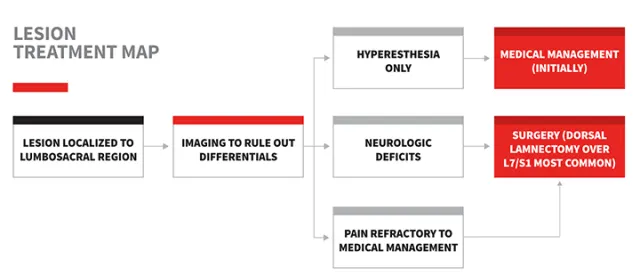
Medical management should be considered initially when pain is the only clinical finding. Essentially, medical management of lumbosacral disease is similar to any protocol for degenerative joint disease/arthritis. Patients should be treated with medications such as NSAIDs and gabapentin. If the patient has had chronic pain, NMDA antagonists such as amantadine can also be considered.
Corticosteroid vs NSAID use in treatment of this disease can be left to the clinician’s preference. The authors prefer to treat with the latter because often a definitive diagnosis is not reached. In addition, the adverse effects of corticosteroids (eg, increase in thirst and urination, increased appetite), may lead to additional movement (urination and defecation) and weight gain.
Medical management should also include modified exercise restriction (eg, short leash walks just long enough for urination/defecation, avoidance of stairs, prevention of running and jumping) because many of these dogs will be working animals. Crate confinement is not strongly recommended for LS disease because it can exacerbate concurrent osteoarthritis. Weight reduction is recommended for overweight patients.
Epidural infiltration of methylprednisolone acetate at the lumbosacral space has been reported. It may be considered because of its minimally invasive nature.10 In a single study of 38 dogs with Hansen type II disk protrusion, 79% of dogs treated with this method were considered to have improved; this is comparable to clinical outcomes for decompressive surgery.10
Patients with moderate-to-severe lumbosacral disease that causes pain unresponsive to medical management and patients with neurologic abnormalities should be considered surgical candidates. The main goal of surgery is decompression of the cauda equina, which can relieve the patient’s pain. Dorsal laminectomy with or without foraminotomy is most often performed.1,5,9,11
Distraction and stabilization may be required to correct ventral subluxation of S1, prevent further lumbosacral instability, or decompress the L7 spinal nerve in the intervertebral foramen. In a single study, an average of 78% of dogs undergoing surgery had an excellent or good outcome, as assessed by both owners and veterinarians.12 Careful preoperative consideration is recommended for patients with urinary and/or fecal incontinence, as surgical resolution of incontinence can be poor. The same study documented that the presence of urinary and/or fecal incontinence before surgery is the only individual clinical sign that significantly affects outcome.12,13
Rehabilitation
Laser, traction, therapeutic ultrasonography, and therapeutic exercises such as underwater treadmills can be considered to aid in recovery and maintain muscle mass.14,15 Rehabilitation can make a significant difference in helping to reduce pain and returning the patient to normal function, with or without surgery.