Polyuria & Polydipsia in a Dog with a Perianal Mass
Julius M. Liptak, BVSc, MVetClinStud, FACVSc, DACVS, DECVS, Alta Vista Animal Hospital

A 10-year-old, 11-kg castrated miniature schnauzer presented with a 4-month history of polyuria and polydipsia.
History
Polyuria and polydipsia were not associated with any other signs. Appetite and activity levels were normal. Clinical history was unremarkable, with no record of recent diseases, surgeries, or medications.
Examination Findings
The dog was alert, responsive, well hydrated, and in good body condition. Thoracic auscultation was normal, with no displacement or muffling of cardiac sounds. Ventral cervical masses were not palpable. Abdominal palpation was unremarkable. A firm mass measuring 4.1 × 5.7 cm was present in the right perianal region (Figure 1). On rectal palpation, a mass was detected in the dorsal sublumbar region.
Diagnostic Results
Hematology findings were within reference ranges. Abnormalities noted on serum biochemistry profile (Table 1) included elevated ALP, ALT, and total calcium. Ionized calcium was also elevated. The only abnormality noted on urinalysis was hyposthenuria (urine specific gravity 1.007; range, 1.015–1.045).
Fine-needle aspiration of the right perianal mass was consistent with apocrine gland anal sac adenocarcinoma (AGASAC).
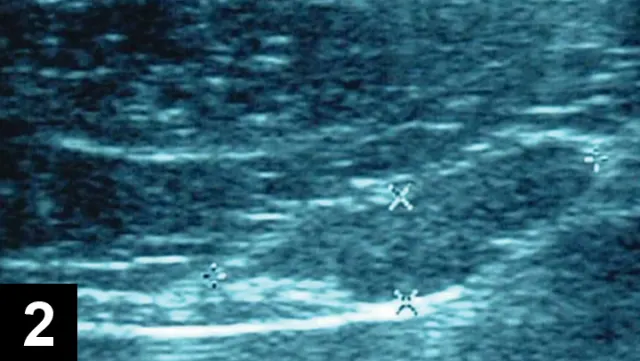
Abdominal ultrasound showing enlarged sublumbar lymph node.
Clinical staging involved 3-view thoracic radiography and abdominal ultrasonography. Evidence of intrathoracic abnormalities, including pulmonary metastasis, was absent on radiographs. Ultrasound abnormalities included an enlarged, heterogenous liver with diffuse multiple hypoechoic foci, moderately enlarged spleen, and an irregular sublumbar lymph node measuring 3 cm in diameter (Figure 2). Ultrasound-guided, fine-needle aspirates of liver and spleen were collected. Cytology of liver aspirates was consistent with steroid hepatopathy (vacuolar degeneration); no abnormalities were noted on cytology of the splenic aspirates.
Ask Yourself
1. What are the differentials for hypercalcemia in dogs?2. What diagnostic measures should be completed to differentiate the various causes of hypercalcemia?3. What are the treatment options for dogs with AGASAC?4. What is the prognosis for dogs with AGASAC?
Diagnosis
AGASAC with hypercalcemia and sublumbar lymph node metastasis
Preliminary Diagnosis
The combination of anal sac mass, enlarged sublumbar lymph node, and hypercalcemia is highly suggestive of unilateral AGASAC with paraneoplastic hypercalcemia and suspected sublumbar lymph node metastasis. Hypercalcemia is reported in 90% of dogs with AGASAC,1,2 because of production of parathyroid hormone-related protein (PTH-rP) by neoplastic cells.
Sublumbar lymph node metastasis is reported in 47% to 72% of dogs with AGASAC.1-4 Removal of the sublumbar lymph nodes is recommended in these dogs because this can significantly improve survival time. For dogs with hypercalcemia, the metastatic lymph node, in addition to primary mass excision, also produces PTH-rP; hence excision of these nodes removes the neoplastic cells and helps resolve the hypercalcemia.
Treatment
In dogs with marked hypercalcemia, saline diuresis will be indicated. Removal of the affected anal sac may resolve mild-to-moderate hypercalcemia when secondary to AGASAC. Sublumbar lymph node excision through exploratory ventral midline celiotomy, followed by unilateral closed anal sacculectomy, was performed. The owners declined adjunctive therapy.
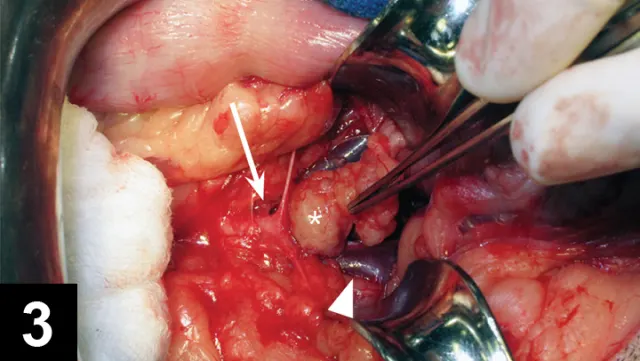
A metastatic sublumbar lymph node (asterisk) extirpated from between the terminal branches of the aorta (arrowhead) and caudal vena cava (arrow).
Sublumbar lymph node excision can be challenging because of poor visibility and regional anatomic structures. Sublumbar lymph nodes are usually located between the terminal branches of the aorta and caudal vena cava; thus, careful dissection of the lymph node is required to avoid disrupting these vessels. The lymph nodes can also extend into the pelvic canal dorsal to the urinary bladder. Dissection is still possible in these cases, but visibility and access can be difficult. In this dog, a 3.5 × 5.5-cm sublumbar lymph node was excised from between the left external iliac artery and vein dorsal to the urinary bladder (Figure 3), and a liver biopsy specimen was collected.
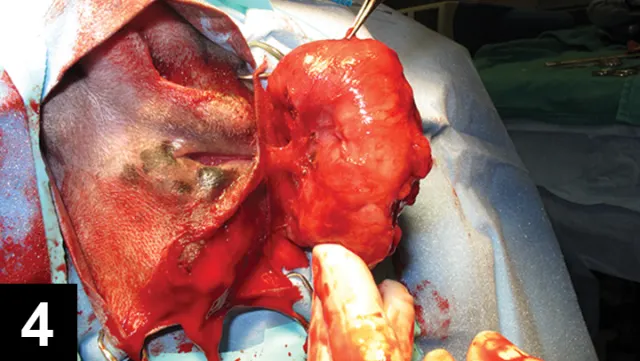
Closed anal sacculectomy for excision of the AGASAC.
Closed sacculectomy was selected (Figure 4), as an open approach is not recommended because it can result in tumor seeding of the perianal space and increase the risk for local tumor recurrence.
Outcome
Hypercalcemia resolved the day after surgery (ionized calcium, 1.38 mmol/L). There were no surgical complications (eg, infection, tenesmus, fecal incontinence). The dog underwent physical examination, rectal palpation, and measurement of ionized calcium monthly for 3 months; testing, abdominal ultrasonography, and three-view thoracic radiography were performed q3mo thereafter. The dog was disease free and normocalcemic 10 months postsurgery.
Did You Answer?
1. Differentials include:
Primary hyperparathyroidism from parathyroid hyperplasia, adenoma, or carcinoma (rare)
Hypercalcemia associated with malignancy (eg, lymphoma, AGASAC, carcinoma, primary and metastatic bone tumors)
Hypoadrenocorticism
Vitamin D toxicity (eg, excessive dietary supplementation, ingestion of cholecalciferol-containing rodenticides or plants)
Chronic renal failure
Miscellaneous causes include osteolytic bone lesions, vitamin A toxicosis, ingestion of calcium carbonate, and spurious increases associated with hyperalbuminemia.
2. Diagnostic measures to differentiate causes of hypercalcemia include:
Palpation for parathyroid masses and thoracic auscultation for displaced and/or muffled cardiac sounds secondary to mediastinal lymphoma
Rectal palpation for AGASAC
Thoracic radiography for the detection of a mediastinal mass
Serum biochemistry to measure total calcium, BUN, and creatinine
Urinalysis for chronic renal failure
Electrolyte measurement for ionized calcium, sodium, and potassium to detect hypoadrenocorticism
If no masses are present on palpation or imaging, ionized calcium, intact parathyroid hormone, PTH-rP, and 25-hydroxyvitamin D levels should be evaluated (Table 2).
3. Treatment options include surgery, chemotherapy, and radiation therapy.Surgery is recommended for excision of the anal sac tumor and metastatic sublumbar lymph nodes (if present). Prognosis is significantly worse without surgery. Chemotherapy options include carboplatin, tyrosine kinase inhibitors (eg, toceranib),6 and metronomic chemotherapy protocols. The median survival time (MST) for surgery alone and for surgery plus adjuvant chemotherapy does not significantly differ.2 Radiation therapy is associated with a numerically, not statistically, superior survival time compared with surgery alone.2
4. The prognosis for dogs with AGASAC can be good.MST was 544 days for treated dogs in a previous study (Tables 3 and 4).2 Presence of sublumbar lymph node metastasis is not a poor prognostic factor if the metastatic lymph node is excised.
AGASAC = apocrine gland anal sac adenocarcinoma, MST = median survival time, PTH-rP = parathyroid hormone-related protein