Orthopedic Examination of the Rearlimb in the Dog
Two of the most common orthopedic conditions causing lameness in the dog affect joints of the pelvic limb: canine hip dysplasia and cranial cruciate ligament disease. These disorders can exist independently or simultaneously. Many other conditions can also be present and somewhat depend on the age, breed, and lifestyle of the dog. As with the forelimb, the rear limb can be divided into anatomic regions to assist with examination: paw, tarsus, tibia/fibula, stifle or knee, femur, hip, and pelvis. Examination should always begin with observing the dog walking to confirm rear limb lameness. Lameness can vary in severity from non–weight-bearing to mild shortness of stride during weight-bearing. The dog should also be examined for postural changes consistent with pelvic limb disorders, such as unwillingness to flex the knee during sitting (the“sit test”) and hyperextension or hyperflexion of the tarsal joint. Neurologic examination should accompany orthopedic examination to rule out other sources of limb dysfunction, such as peripheral neuropathies or, more commonly, intervertebral disc disease and lumbosacral disease.
STEP BY STEP ORTHOPEDIC EXAMINATION OF THE REAR LIMB


1. The Paw
Examination of the paw generally consists of examining each individual digit, including the nail and nail bed (A). Common sources of lameness arising from these sites include split nails, nail-bed tumors, fracture/luxation of the phalanges, penetrating foreign bodies, and pad lacerations. Careful palpation of the digits and manipulation of the joints in flexion and extension (B, C), while observing for evidence of pain or swelling, make up a fairly sensitive method to determine whether any part of the paw is a source of pain. Injury to the paw or digits is a frequent source of non–weightbearing lameness. Because many dogs are sensitive to having their paws handled, the examiner should also palpate the feet from the unaffected legs to gain a sense of the level of an animal’s reluctance to having its paws manipulated.

2. The Tarsus
Of the 4 joints that make up the tarsus, only the tibiotarsal joint exhibits appreciable motion in flexion and extension as a hinge joint. Any of the joints can be compromised by trauma, with resulting laxity in directions associated with the damaged stabilizing structures. The tarsal joints should be palpated and stressed in medial and lateral directions, as well as in flexion (A) and extension (B), to assess for excessive laxity indicating subluxations or luxations. The tibiotarsal joint should be palpated through its normal range of motion to feel for crepitus or popping. The latter can occur with displacement of the superficial digital flexor tendon, which occurs with associated retinaculum tearing during overuse injuries and can cause hyperflexion of the tarsus and digits. Another reason for a dropped or hyperflexed tibiotarsal joint is damage to the common calcaneal tendon. This structure should be palpated from its insertion on the calcaneus proximally to assess for disruption, inflammation, or fibrosis associated with injury. The various tarsal bones can fracture, causing pain and inflammation. Young large-breed dogs should be examined closely for swelling in the tibiotarsal joint, which may be consistent with osteochondritis dissecans. Distension of the joint capsule is palpable on the dorsal surface, as well as caudomedial and caudolateral aspects (C). Joint swelling in adult animals may be attributable to degenerative joint disease or the various causes of suppurative arthritis.
3. The Tibia & Fibula
Sources of lameness in young dogs that can arise from the tibia and fibula include hypertrophic osteodystrophy, eosinophilic panosteitis, Salter-Harris fractures, and physeal disturbances; and in young adult and adult dogs other fractures, neoplasia, angular limb deformities, and hypertrophic osteopathy. Examination of the tibia should focus on deep palpation to elicit an osseus source of pain or detect focal areas of swelling. The relationship of the tarsus to the stifle should also be observed for evidence of angulation from physeal damage and abnormal development of the tibia and fibula. Aberrant growth from physeal disturbances can result in varus, valgus, procurvatum,recurvatum, or rotational or translational deformities.
PROCEDURE PEARL
Examination of the tibia should focus on deep palpation to elicit an osseus source of pain or detect focal areas of swelling.

4. The Stifle
The stifle is a very common source of lameness in the dog. Young dogs can be in pain from osteochondritis and patellar luxations, whereas older dogs can be in pain from cranial cruciate ligament disease, caudal cruciate ligament tears, collateral instability, patellar luxation, meniscal disease, and long digital extensor tendon injuries.
Examination While StandingE

xamination of the stifle can begin with the animal standing, a position that allows simultaneous palpation of the knees bilaterally. This is particularly useful for comparison if the animal has the condition unilaterally. Specifically, the edges of the patellar tendon should be distinguished because loss of palpable edges to this structure is consistent with effusion (A). The proximal medial aspect of both tibias is palpated for evidence of a hard, round swelling called a fibrous “buttress,” which occurs with cranial cruciate ligament disease (B). The position of the patella is also determined to identify the presence and direction of a patellar luxation.
E__xamination in Lateral RecumbencyThe remainder of the stifle examination is done with the dog in lateral recumbency. Palpation of the stifle typically begins with putting the joint through its full range of motion, which should be easily accomplished without crepitus or pain. Clicking or popping may indicate meniscal tears. The integrity of the cranial cruciate ligament is examined through an active, cranial tibial thrust
maneuver and a passive cranial drawer test. For the former, the stifle is held at a fixed angle and the hock is flexed while palpating for cranial subluxation of the proximal tibia at the level of the tibial tuberosity (C). With the latter test, the femur is grasped at the lateral fabella and patella and the tibia is grasped at the caudal-proximal aspect and tibial crest while the examiner attempts to translate the tibia cranially (D). The stifle can then be placed under stress both medially and laterally to assess both collateral ligaments. The patella should be reassessed with the dog in lateral recumbency while the tibia is rotated both internally and externally to determine whether medial or lateral laxity is present (E).
PROCEDURE PEARL
A common tumor of the canine rear limb is osteosarcoma, which more frequently forms in the distal femur and proximal tibia.
5. The Femur
Conditions potentially affecting the femur include panosteitis, hypertrophic osteodystrophy, and fractures in the young dog and fractures, neoplasia, and hypertrophic osteopathy in the adult dog. A common tumor of the canine rear limb is osteosarcoma, which more frequently forms in the distal femur and proximal tibia. Examination should include deep palpation along the length of the femur to examine for pain, inflammation, or swelling.


6. The Hip
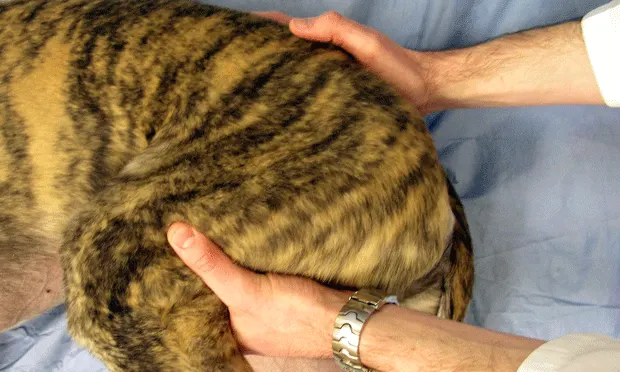
Causes of pain in the canine hip include hip dysplasia with laxity, avascular necrosis, luxations, and fractures in the young animal; and hip dysplasia with secondary degenerative joint disease, luxations, suppurative arthropathies, neoplasia, and fractures in the adult dog. Examination of the hip starts by putting the joint through its full range of motion, including flexion (A) and extension (B), while observing for pain or palpable crepitus. Young dogs should then be examined for hip laxity as a sign of the early phase of canine hip dysplasia. Although many palpation maneuvers exist, one of the most common techniques is the Ortolani examination. To perform this, the dog will probably need to be lightly sedated and may be placed in dorsal or lateral recumbency.

The stifle and hip should both be at 90° of flexion. A compressive force is applied along the axis of the femur, with one hand at the level of the stifle, while a countercompressive force is applied over the hip and pelvis with the opposite hand (C). The thumb of this hand should be placed over the greater trochanter to feel for subluxation and reduction. If hip laxity is present, the femoral head will have subluxated slightly during this phase. While the axial force is applied, the leg is abducted slowly while the trochanter is palpated (D) and the Ortolani sign is sought: a palpable clunk signifying the reduction of the head into the acetabulum.

7. The Pelvis
Painful conditions of the pelvis include fractures, luxations of the sacroiliac joint, and neoplasia. Palpation of the pelvis can be paired with palpation of the proximal femur. The appropriate relationship between pelvis and femur can be documented by the palpation of the wing of the ilium, ischial tuberosity, and greater trochanter, which should form a triangle (photo). If the triangular shape is lost, hip luxations should be suspected. Most pelvic fractures will be definitively diagnosed by using radiographs but they may first be detected through rectal palpation. The latter will allow assessment of the ventral pubic symphysis ventrally and medial walls of the acetabulum, depending on size of the dog.
Conclusion
As with the forelimb, observation of gait, neurologic examination, and systematic palpation of specific anatomic structures will help elucidate many orthopedic conditions of the rear limb. Most often, presumptive diagnoses based on orthopedic examination should be followed up with specific imaging modalities to confirm the diagnosis and provide clients with treatment options and prognoses.
Acknowledgment:The author wishes to thank Dr. David Dismukes for his assistance in preparing the figures.