
Anisocoria represents unilateral or asymmetric ocular or nervous system pathology. To determine the significance of anisocoria, normal functions of the iris must be recognized. The iris sphincter and dilator muscles are innervated by parasympathetic and sympathetic neurons, respectively. These antagonistic muscles are responsible for controlling pupil size, which in turn determines the amount of light reaching the retina.
Anisocoria can manifest from a variety of lesions that occur locally in the eye or along neurologic tracts that supply innervation to the iris sphincter and dilator muscles. These lesions can result in inappropriate miosis or mydriasis.
Subtle differences can make determining the abnormal pupil difficult. Assessing vision and pupillary light reflexes, as well as increasing or decreasing room lighting, can be helpful:
Increased room lighting can enhance parasympathetic lesions by causing the unaffected pupil to constrict, which cannot occur in the affected eye due to decreased parasympathetic innervation.
Decreased room lighting can enhance sympathetic lesions by allowing the unaffected pupil to dilate, which cannot occur in the affected eye due to decreased sympathetic innervation.1
If a lesion is determined to be neurologic (Figures 1-2), advanced imaging (eg, CT, MRI) is generally helpful to establish the specific location and/or particular cause of the lesion.2 A variety of diagnostic testing and imaging may be necessary, particularly when conditions with significant impacts on health are suspected.
Anisocoria findings should always be interpreted with history and results from complete ophthalmic and neurologic examinations (Figure 3); treatment should be directed toward the underlying cause, if identified. Some common ocular causes of anisocoria include:
Anterior uveitis
Congenital iris anomalies
Asymmetric iris atrophy
Glaucoma
This anisocoria image gallery focuses on the neuroanatomic pathways of pupillary control and reviews some common clinical causes of anisocoria; ocular causes are covered first, followed by nonocular (including neurologic) causes.
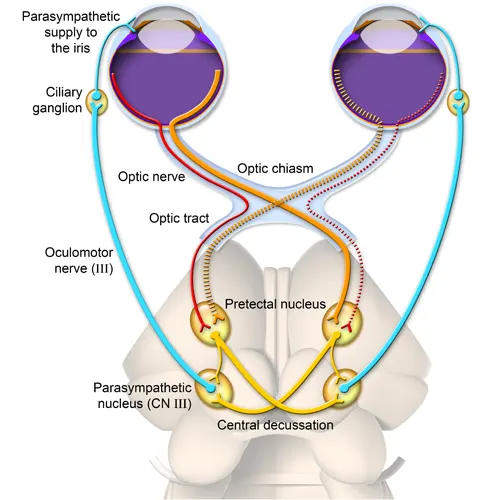
FIGURE 1 Illustration of parasympathetic innervation to the iris
Parasympathetic preganglionic fibers begin in the parasympathetic nucleus of cranial nerve III (oculomotor nerve; blue line), which receives information from vision pathways. These fibers pass through the cavernous sinus before entering the orbit and synapsing at the ciliary ganglion. Postganglionic fibers then enter the globe. Denervation along this pathway may result in anisocoria, with an affected pupil being more dilated than a normal pupil. Lesions affecting the oculomotor nerve can result in ventrolateral strabismus, external ophthalmoplegia (ie, paralysis of extraocular muscles), and ptosis, as the oculomotor nerve innervates several extraocular muscles and the levator palpebrae superioris muscle.2 CN = cranial nerve